

Fibular strut allograft influences reduction and outcomes after locking plate fixation of comminuted proximal humeral fractures in elderly patients: a retrospective study
- PMID: 31679513
- PMCID: PMC6825724
- DOI: 10.1186/s12891-019-2907-3
Fibular strut allograft influences reduction and outcomes after locking plate fixation of comminuted proximal humeral fractures in elderly patients: a retrospective study
Abstract
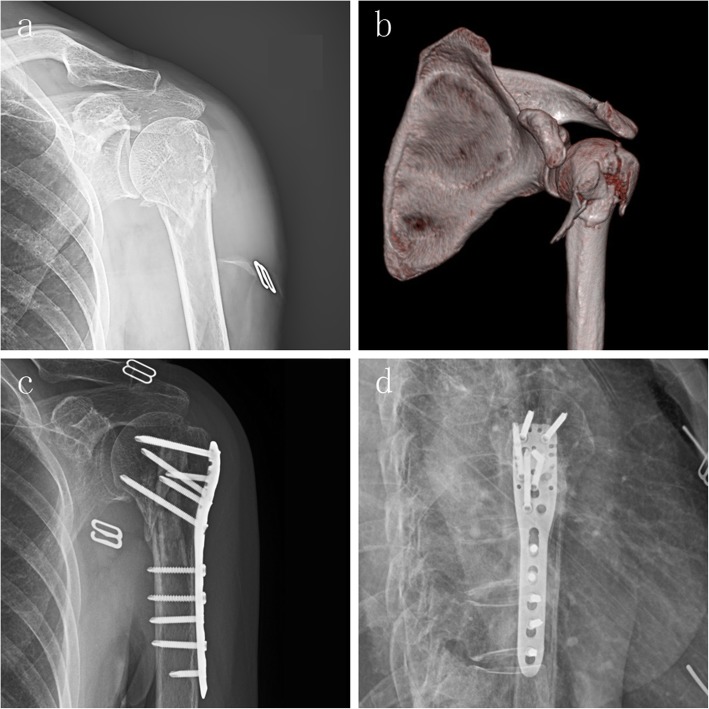
Background: Proximal humeral fractures (PHFs) are the third most commonly occurring fractures in elderly patients. Most of these fractures can be treated with conservative methods, but the optimal surgical treatment strategy for unstable fractures in elderly patients remains controversial. This study aimed to compare the radiological and clinical outcomes between locking compression plate (LCP) fixation and LCP fixation with fibular allograft implantation for the treatment of comminuted PHFs.
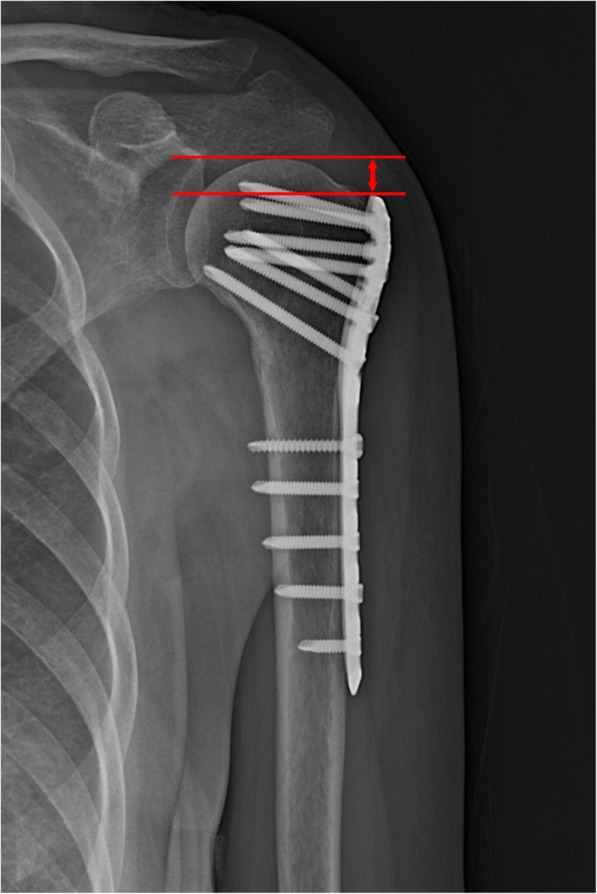
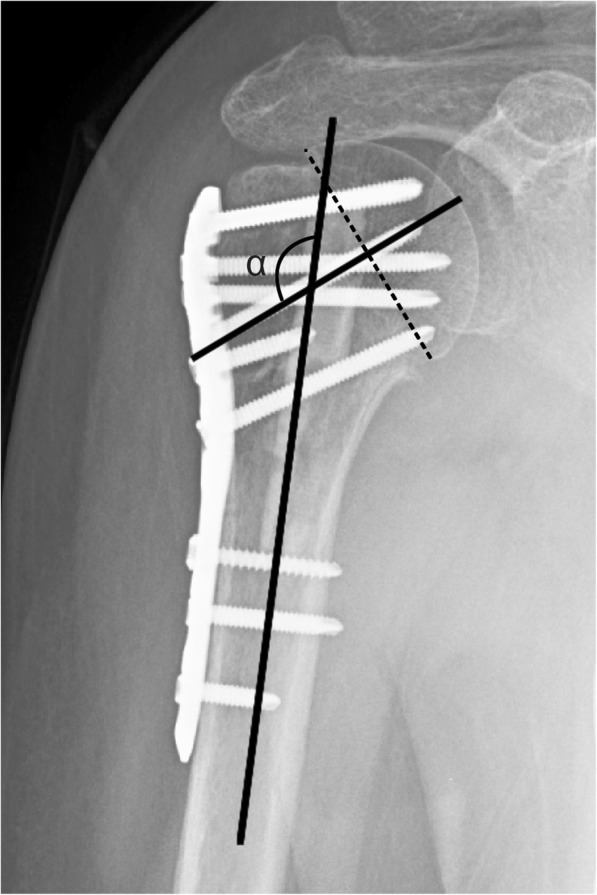
Methods: We retrospectively reviewed 60 patients (mean age, 72.75 years) with closed 3- or 4-part fractures, and a minimum of 2 years of follow-up. Fracture reduction was quantitatively determined by humeral head height (HHH) and neck-shaft angle (NSA). The clinical outcome was evaluated by Constant-Murley score (CMS) and American Shoulder and Elbow Surgeons (ASES) score.
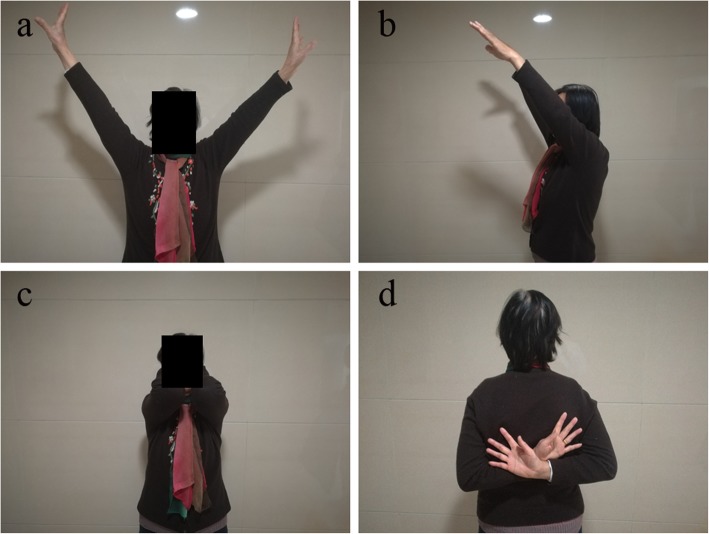
Result: The average radiological changes were higher in the LCP group than in the locking plate with fibular allograft group (HHH of 4.16 mm vs 1.18 mm [p < 0.001] and NSA of 9.94° versus 3.12° [p < 0.001]) . The final average outcome scores were lower in the LCP group than in the FA group (CMS of 73.00 vs 78.96 [p = 0.024] and ASES score of 72.80 vs 78.64 [p = 0.022]). The FA group showed better forward elevation (p = 0.010) and abduction (p = 0.002); however, no significant differences were observed for shoulder external rotation or internal rotation. The number of complications was higher in the LCP group (28.57%) than in the FA group (1.2%) (p < 0.001).
Conclusion: For comminuted PHFs in elderly patients, LCP fixation combined with a fibular allograft is reasonable option to ensure satisfactory radiological and clinical outcomes.
Trial registration: ZDYJLY(2018)New-9 . Name of registry: IEC for clinical Research of Zhongda Hospital, Affiliated to Southeast University. Date of registration: 2018-05-17.
Keywords: Elderly patients; Fibular allograft; Locking plate; Proximal humeral fracture.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures
References
-
- Neer CS 2nd Displaced proximal humeral fractures. Part I. Classification and evaluation. Clin Orthop Relat Res. 2006;442:77–82. doi: 10.1097/01.blo.0000198718.91223.ca. - DOI - PubMed
-
- Walsh S, Reindl R, Harvey E, Berry G, Beckman L, Steffen T. Biomechanical comparison of a unique locking plate versus a standard plate for internal fixation of proximal humerus fractures in a cadaveric model. Clin Biomech (Bristol, Avon) 2006;21(10):1027–1031. doi: 10.1016/j.clinbiomech.2006.06.005. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
