

Liver Fat and Cardiometabolic Risk Factors Among School-Age Children
- PMID: 31680281
- PMCID: PMC7496381
- DOI: 10.1002/hep.31018
Liver Fat and Cardiometabolic Risk Factors Among School-Age Children
Abstract
Background and aims: Nonalcoholic fatty liver disease is a major risk factor for cardiometabolic disease in adults. The burden of liver fat and associated cardiometabolic risk factors in healthy children is unknown. In a population-based prospective cohort study among 3,170 10-year-old children, we assessed whether both liver fat accumulation across the full range and nonalcoholic fatty liver disease are associated with cardiometabolic risk factors already in childhood.
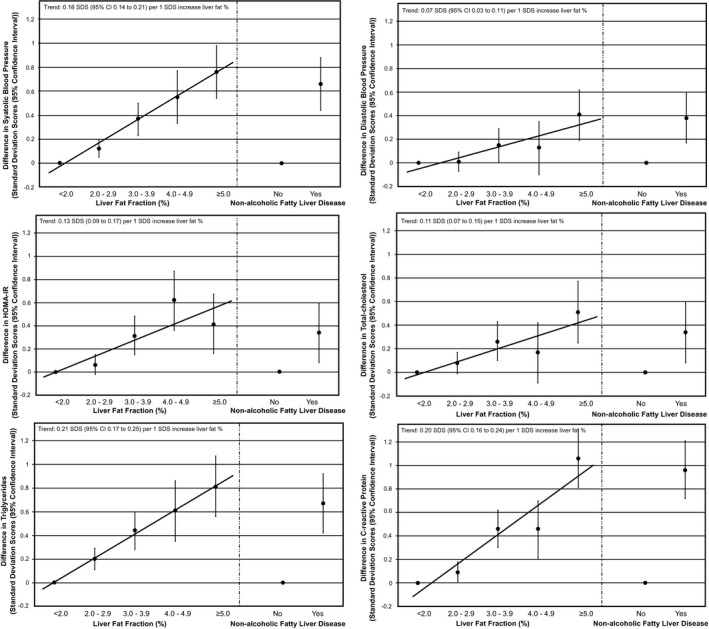
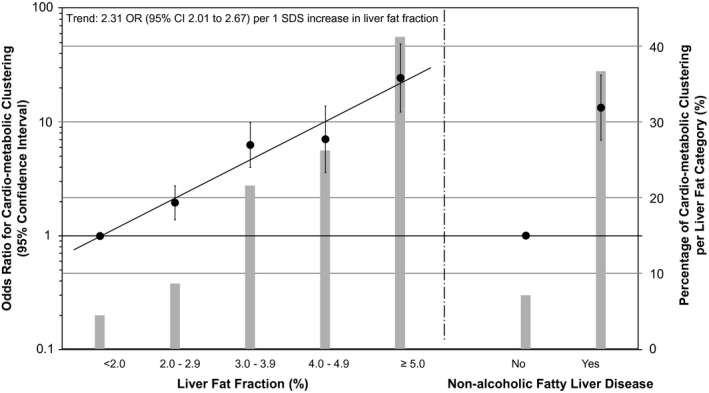
Approach and results: Liver fat fraction was measured by magnetic resonance imaging, and nonalcoholic fatty liver disease was defined as liver fat fraction ≥5.0%. We measured body mass index, blood pressure, and insulin, glucose, lipids, and C-reactive protein concentrations. Cardiometabolic clustering was defined as having three or more risk factors out of high visceral fat mass, high blood pressure, low high-density-lipoprotein cholesterol or high triglycerides, and high insulin concentrations. Nonalcoholic fatty liver disease prevalences were 1.0%, 9.1%, and 25.0% among children who were normal weight, overweight, and obese, respectively. Both higher liver fat within the normal range (<5.0% liver fat) and nonalcoholic fatty liver disease were associated with higher blood pressure, insulin resistance, total cholesterol, triglycerides, and C-reactive protein concentrations (P values < 0.05). As compared with children with <2.0% liver fat, children with ≥5.0% liver fat had the highest odds of cardiometabolic clustering (odds ratio 24.43 [95% confidence interval 12.25, 48.60]). The associations remained similar after adjustment for body mass index and tended to be stronger in children who were overweight and obese.
Conclusions: Higher liver fat is, across the full range and independently of body mass index, associated with an adverse cardiometabolic risk profile already in childhood. Future preventive strategies focused on improving cardiometabolic outcomes in later life may need to target liver fat development in childhood.
© 2019 The Authors. Hepatology published by Wiley Periodicals, Inc. on behalf of American Association for the Study of Liver Diseases.
Figures
References
-
- Targher G, Day CP, Bonora E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N Engl J Med 2010;363:1341‐1350. - PubMed
-
- Bedogni G, Gastaldelli A, Manco M, De Col A, Agosti F, Tiribelli C, et al. Relationship between fatty liver and glucose metabolism: a cross‐sectional study in 571 obese children. Nutr Metab Cardiovasc Dis 2012;22:120‐126. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
