

Immunotherapy for head and neck cancer: Recent advances and future directions
- PMID: 31683169
- PMCID: PMC7749717
- DOI: 10.1016/j.oraloncology.2019.104460
Immunotherapy for head and neck cancer: Recent advances and future directions
Abstract
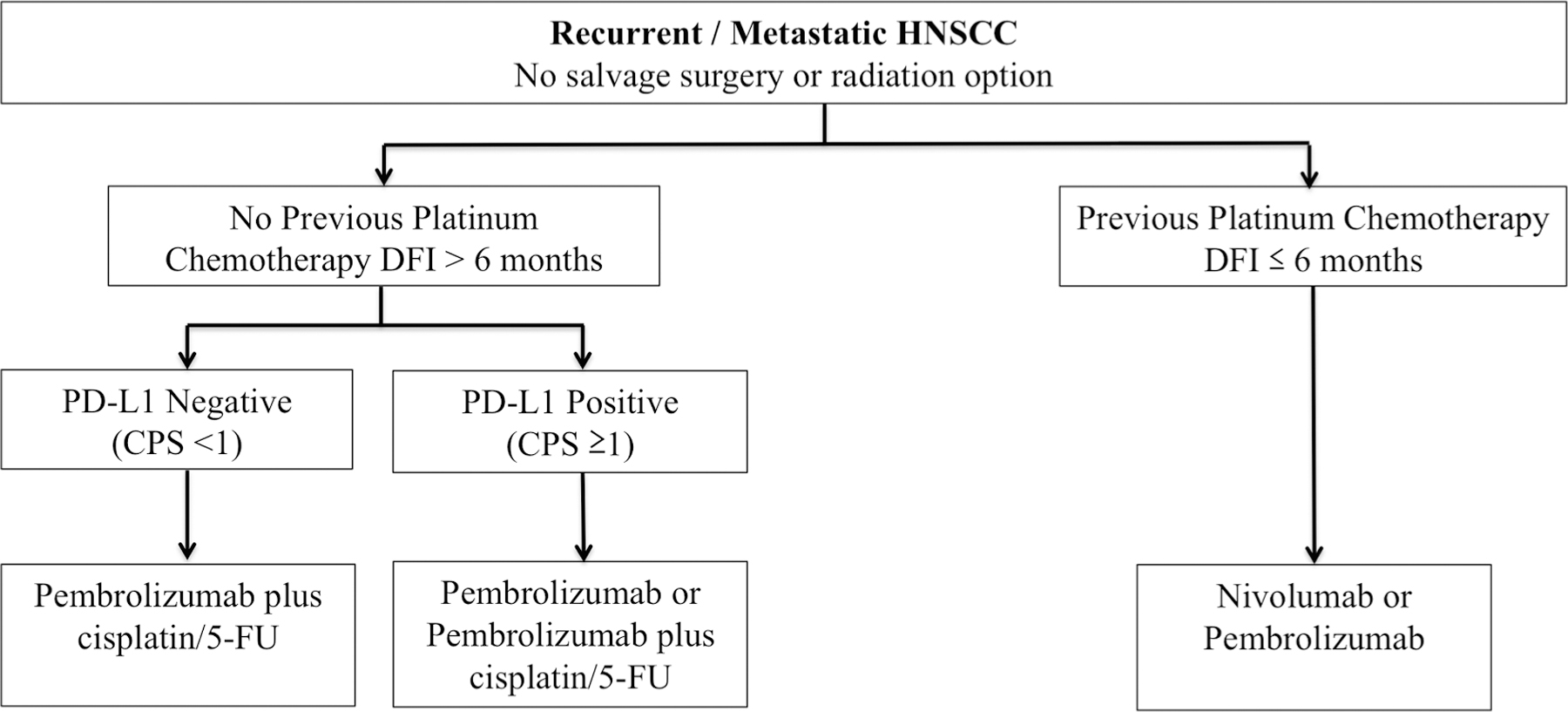
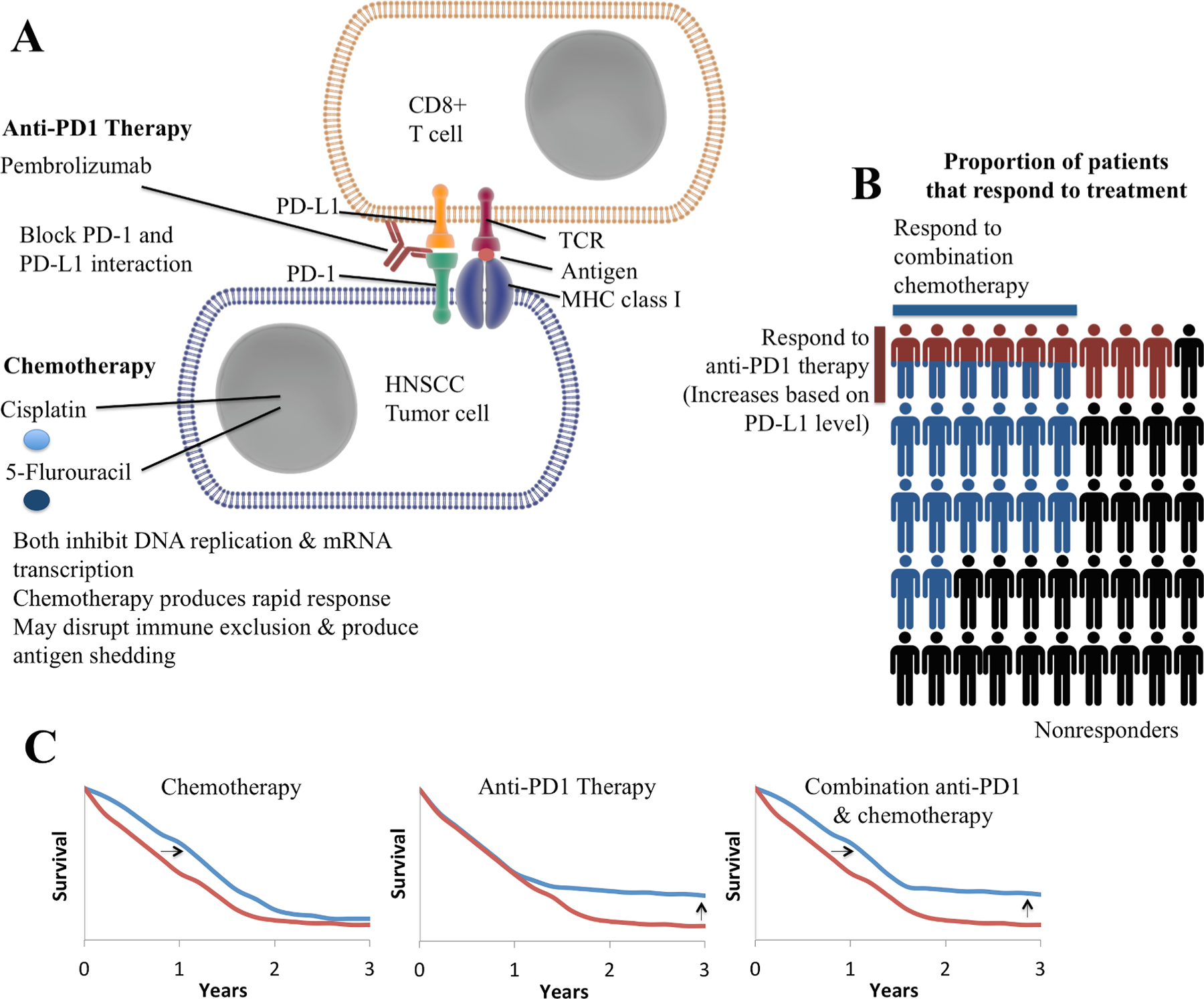
Three randomized phase III trials have now conclusively proven that exposure to a PD-1 inhibitor prolongs survival in recurrent/metastatic (R/M) HNSCC, and it is clear that such agents should be used in the management of all patients who do not have contraindications to their use. Two of these phase III randomized trials showed that the anti-PD1 antibodies nivolumab and pembrolizumab were superior to investigators' choice chemotherapy in second-line platinum-refractory R/M HNSCC. Recently, a third phase III randomized trial, KEYNOTE-048, showed that pembrolizumab with chemotherapy was superior to the EXTREME regimen (cis- or carboplatin, 5-fluorouracil (5-FU) and cetuximab) in all patients, and pembrolizumab monotherapy was superior in patients whose tumors express PD-L1 in first-line R/M HNSCC. Pembrolizumab is now approved as monotherapy in PD-L1 expressing disease (combined positive score ≥1) or in combination with chemotherapy for all patients with R/M HNSCC. Thus, PD-L1 biomarker testing will be routinely used in R/M HNSCC, and this employs a scoring system that incorporates immune cell staining, referred to as the combined positive score (CPS). Additionally, for the 85% of patients with PD-L1 CPS ≥1, clinical judgment will guide the choice of pembrolizumab monotherapy or pembrolizumab plus chemotherapy, until more detailed clinical data are forthcoming to better inform this decision. In this article we discuss the clinical trials leading to these therapeutic advances and we will review initial results from clinical trials in previously untreated, locally advanced disease, and those using novel combinations of checkpoint inhibitors, co-stimulatory agonists, and therapeutic vaccines.
Keywords: Head and neck cancer; Head and neck squamous cell carcinoma; Immune checkpoint inhibitor; Immunotherapy; Nivolumab; Pembrolizumab.
Copyright © 2019. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest
The authors declared that there is no conflict of interest.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Leemans CR, Braakhuis BJ, Brakenhoff RH. The molecular biology of head and neck cancer. Nat Rev Cancer 2011;11:9–22. - PubMed
-
- Vermorken JB, Mesia R, Rivera F, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med 2008;359:1116–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
