

Screening for Colorectal Cancer in Asymptomatic Average-Risk Adults: A Guidance Statement From the American College of Physicians
- PMID: 31683290
- PMCID: PMC8152103
- DOI: 10.7326/M19-0642
Screening for Colorectal Cancer in Asymptomatic Average-Risk Adults: A Guidance Statement From the American College of Physicians
Erratum in
-
Correction: Screening for Colorectal Cancer in Asymptomatic Average-Risk Adults.Ann Intern Med. 2020 Apr 7;172(7):512. doi: 10.7326/L20-0137. Ann Intern Med. 2020. PMID: 32252082 No abstract available.
-
Correction: Previously Undisclosed Potential Conflict of Interest by an Author of American College of Physicians Clinical Guidelines.Ann Intern Med. 2023 Apr;176(4):584. doi: 10.7326/L23-0043. Epub 2023 Feb 14. Ann Intern Med. 2023. PMID: 36780651 No abstract available.
Abstract
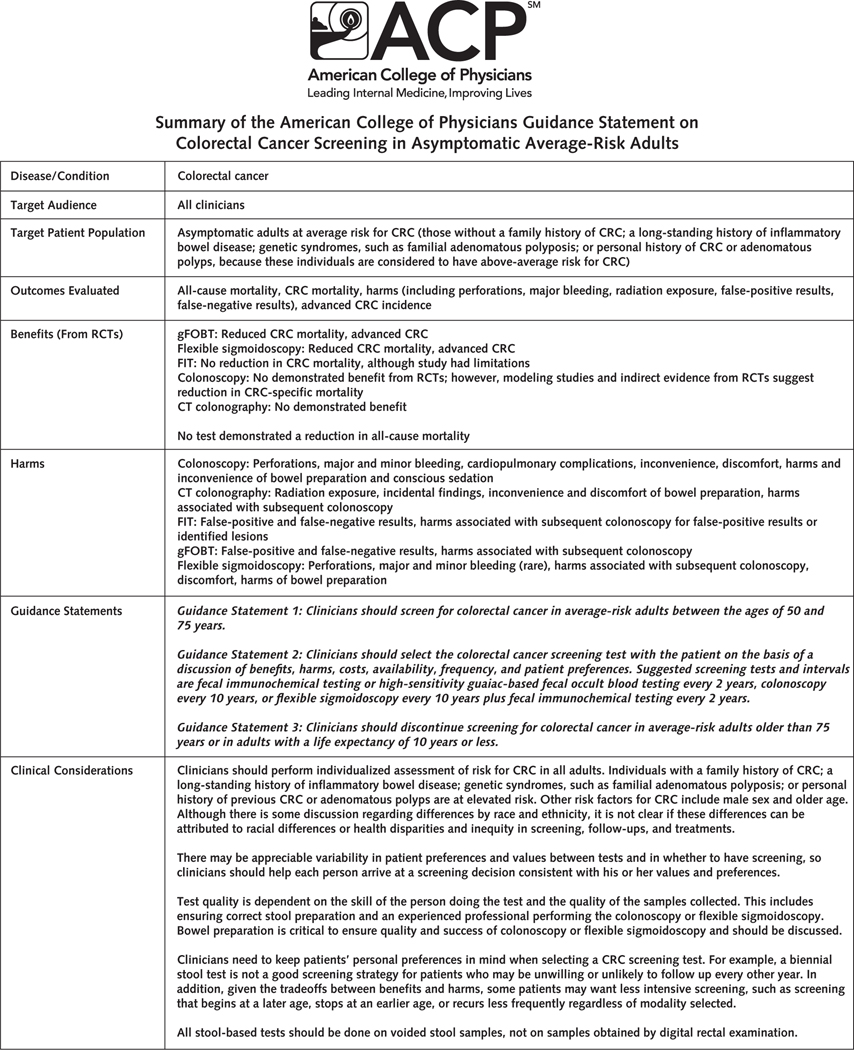
Description: The purpose of this guidance statement is to guide clinicians on colorectal cancer screening in average-risk adults.
Methods: This guidance statement is derived from a critical appraisal of guidelines on screening for colorectal cancer in average-risk adults and the evidence presented in these guidelines. National guidelines published in English between 1 June 2014 and 28 May 2018 in the National Guideline Clearinghouse or Guidelines International Network library were included. The authors also included 3 guidelines commonly used in clinical practice. Web sites were searched for guideline updates in December 2018. The AGREE II (Appraisal of Guidelines for Research and Evaluation II) instrument was used to evaluate the quality of guidelines.
Target audience and patient population: The target audience is all clinicians, and the target patient population is adults at average risk for colorectal cancer.
Guidance statement 1: Clinicians should screen for colorectal cancer in average-risk adults between the ages of 50 and 75 years.
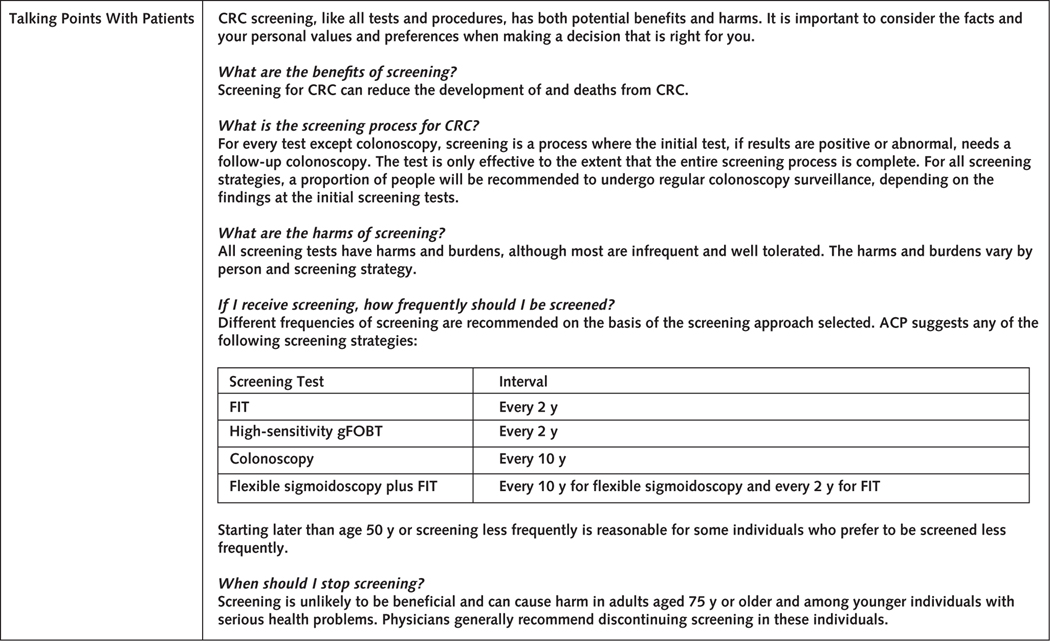
Guidance statement 2: Clinicians should select the colorectal cancer screening test with the patient on the basis of a discussion of benefits, harms, costs, availability, frequency, and patient preferences. Suggested screening tests and intervals are fecal immunochemical testing or high-sensitivity guaiac-based fecal occult blood testing every 2 years, colonoscopy every 10 years, or flexible sigmoidoscopy every 10 years plus fecal immunochemical testing every 2 years.
Guidance statement 3: Clinicians should discontinue screening for colorectal cancer in average-risk adults older than 75 years or in adults with a life expectancy of 10 years or less.
Conflict of interest statement
Figures
Comment in
-
Screening for Colorectal Cancer in Asymptomatic Average-Risk Adults.Ann Intern Med. 2020 Apr 7;172(7):506-507. doi: 10.7326/L20-0112. Ann Intern Med. 2020. PMID: 32252078 No abstract available.
-
Screening for Colorectal Cancer in Asymptomatic Average-Risk Adults.Ann Intern Med. 2020 Apr 7;172(7):507-508. doi: 10.7326/L20-0113. Ann Intern Med. 2020. PMID: 32252079 No abstract available.
-
Screening for Colorectal Cancer in Asymptomatic Average-Risk Adults.Ann Intern Med. 2020 Apr 7;172(7):508. doi: 10.7326/L20-0114. Ann Intern Med. 2020. PMID: 32252080 No abstract available.
-
Screening for Colorectal Cancer in Asymptomatic Average-Risk Adults.Ann Intern Med. 2020 Apr 7;172(7):508-509. doi: 10.7326/L20-0115. Ann Intern Med. 2020. PMID: 32252081 No abstract available.
References
-
- Qaseem A, Kansagara D, Lin JS, et al. ; Clinical Guidelines Committee of the American College of Physicians. The development of clinical guidelines and guidance statements by the Clinical Guidelines Committee of the American College of Physicians: update of methods. Ann Intern Med. 2019;170:863–70. [PMID: 31181568] doi: 10.7326/M18-3290 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical