

2017 ACC/AHA Blood Pressure Classification and Cardiovascular Disease in 15 Million Adults of Age 20-94 Years
- PMID: 31683957
- PMCID: PMC6912685
- DOI: 10.3390/jcm8111832
2017 ACC/AHA Blood Pressure Classification and Cardiovascular Disease in 15 Million Adults of Age 20-94 Years
Abstract
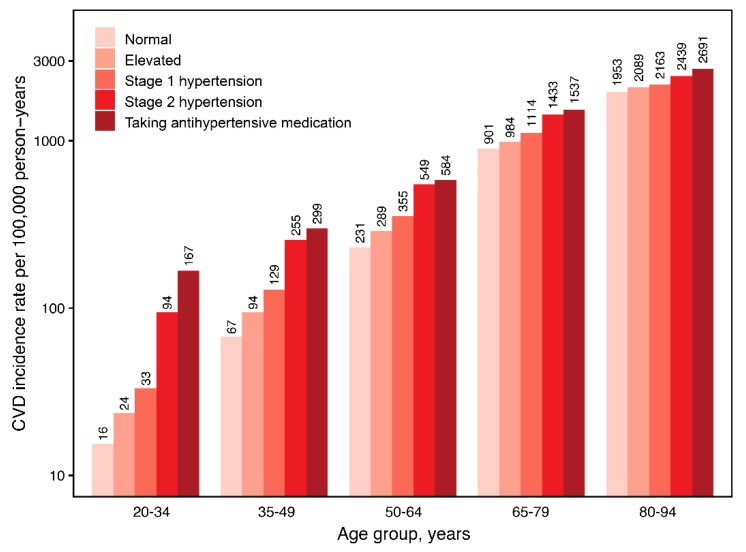
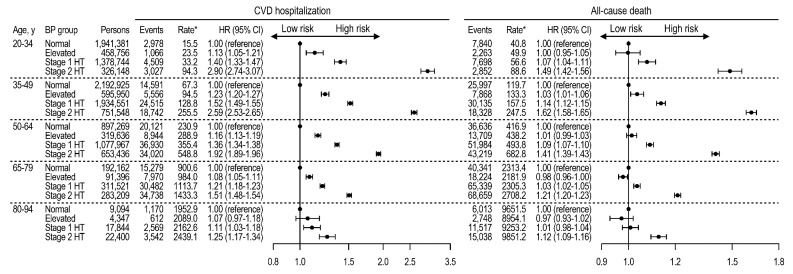
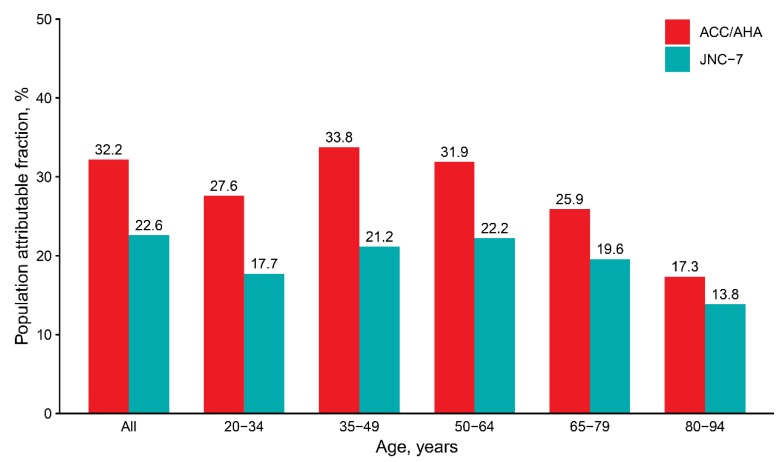
The 2017 American College of Cardiology/American Heart Association (ACC/AHA) high blood pressure (BP) guideline lowered the cut-off for hypertension, but its age-specific association with cardiovascular disease (CVD) remains inconclusive in different populations. We evaluated the association between high BP according to the 2017 ACC/AHA guideline and CVD risks in Koreans aged 20-94 years. In a nationwide health screening cohort, we included 15,508,537 persons aged 20-94 years without prior CVD. BP was categorized into normal, elevated, stage 1 hypertension, or stage 2 hypertension. The primary outcome was a composite CVD hospitalization (myocardial infarction, stroke, and/or heart failure). Over 10 years of follow-up, CVD incidence rates per 100,000 person-years were 105.4, 168.3, 215.9, and 641.2 for normal, elevated BP, stage 1, and stage 2 hypertension, respectively. The age-specific hazard ratios of stage 1 hypertension compared to normal BP were 1.41 (1.34-1.48) at ages 20-34, 1.54 (1.51-1.57) at ages 35-49, 1.38 (1.35-1.40) at ages 50-64, 1.21 (1.19-1.24) at ages 65-79, and 1.11 (1.03-1.19) at ages 80-94 years. With the lowered BP cut-off, 130/80 mmHg, population attributable fraction for CVD was 32.2%. In conclusion, stage 1 hypertension was significantly associated with a higher CVD risk across entire adulthood. The new definition of hypertension may have a substantial population impact on primary CVD prevention.
Keywords: age-specific risk; guideline; hypertension; population attributable risk; real world data.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Whelton P.K., Carey R.M., Aronow W.S., Casey D.E., Jr., Collins K.J., Dennison Himmelfarb C., DePalma S.M., Gidding S., Jamerson K.A., Jones D.W., et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American college of cardiology/American heart association task force on clinical practice guidelines. J. Am. Coll. Cardiol. 2018;71:e127–e248. - PubMed
-
- Khera R., Lu Y., Lu J., Saxena A., Nasir K., Jiang L., Krumholz H.M. Impact of 2017 ACC/AHA guidelines on prevalence of hypertension and eligibility for antihypertensive treatment in United States and China: Nationally representative cross sectional study. BMJ. 2018;362:k2357. doi: 10.1136/bmj.k2357. - DOI - PMC - PubMed
-
- Goff D.C., Lloyd-Jones D.M., Bennett G., Coady S., D’Agostino R.B., Gibbons R., Greenland P., Lackland D.T., Levy D., O’Donnell C.J., et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American college of cardiology/American heart association task force on practice guidelines. Circulation. 2014;129:S49–S73. doi: 10.1161/01.cir.0000437741.48606.98. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
