

Bilateral adrenal hemorrhage after hip arthroplasty: an initially misdiagnosed case
- PMID: 31684918
- PMCID: PMC6829824
- DOI: 10.1186/s12894-019-0536-7
Bilateral adrenal hemorrhage after hip arthroplasty: an initially misdiagnosed case
Abstract
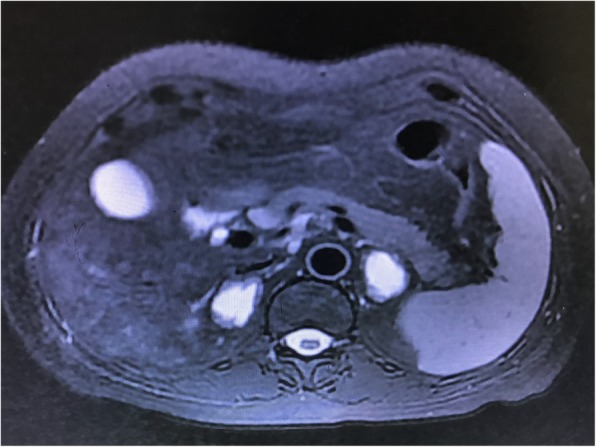
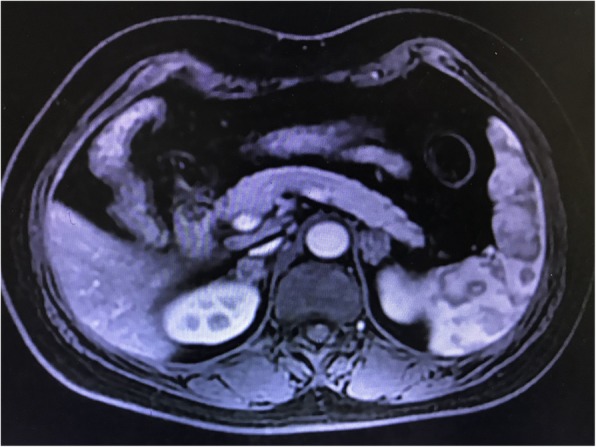
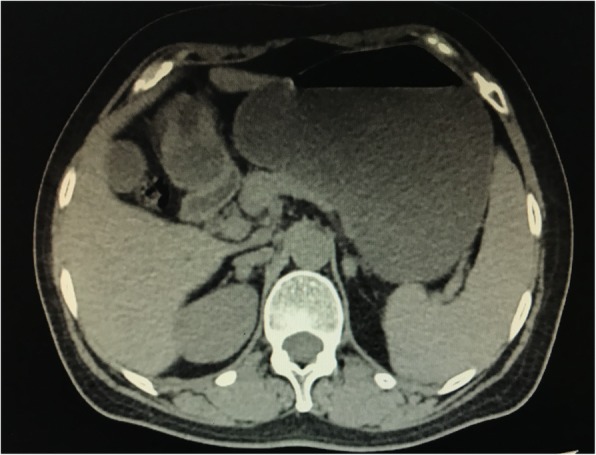
Background: Bilateral adrenal hemorrhage (BAH) is a rare but potentially catastrophic condition. Its clinical manifestation is often non-specific and sometimes difficult to be diagnosed in time. A 57-year-old woman, who presented with severe fatigue, nausea and vomiting after left hip arthroplasty due to her femoral neck fracture in a local hospital, was transferred to our medical center. Laboratory results revealed significant hyponatremia, low serum cortisol and elevated serum ACTH. Computed tomography (CT) showed a bilateral adrenal mass, measured 3.6 × 2.7 cm on the left and 3.4 × 2.3 cm on the right. Further magnetic resonance imaging (MRI) confirmed the diagnosis of BAH. The patient was prescribed with oral prednisolone acetate, 5 mg, tid, and her condition improved gradually. Nine months after, the patient was in good condition with 5 mg prednisolone acetate per day. CT revealed a clearly shrunken adrenal mass compared with 9 months ago.
Conclusions: This case illustrates the difficulty in making the diagnosis of BAH with atypical presentation. Such cases necessitate greater alertness on the part of the clinician and require rapid diagnosis and prompt glucocorticoid replacement for better clinical outcomes.
Keywords: Anticoagulants; Arthroplasty; Bilateral adrenal hemorrhage; Case report; Glucocorticoid replacement; Stress.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
