

Diagnosed prevalence of Ehlers-Danlos syndrome and hypermobility spectrum disorder in Wales, UK: a national electronic cohort study and case-control comparison
- PMID: 31685485
- PMCID: PMC6858200
- DOI: 10.1136/bmjopen-2019-031365
Diagnosed prevalence of Ehlers-Danlos syndrome and hypermobility spectrum disorder in Wales, UK: a national electronic cohort study and case-control comparison
Abstract
Objectives: To describe the epidemiology of diagnosed hypermobility spectrum disorder (HSD) and Ehlers-Danlos syndromes (EDS) using linked electronic medical records. To examine whether these conditions remain rare and primarily affect the musculoskeletal system.
Design: Nationwide linked electronic cohort and nested case-control study.
Setting: Routinely collected data from primary care and hospital admissions in Wales, UK.
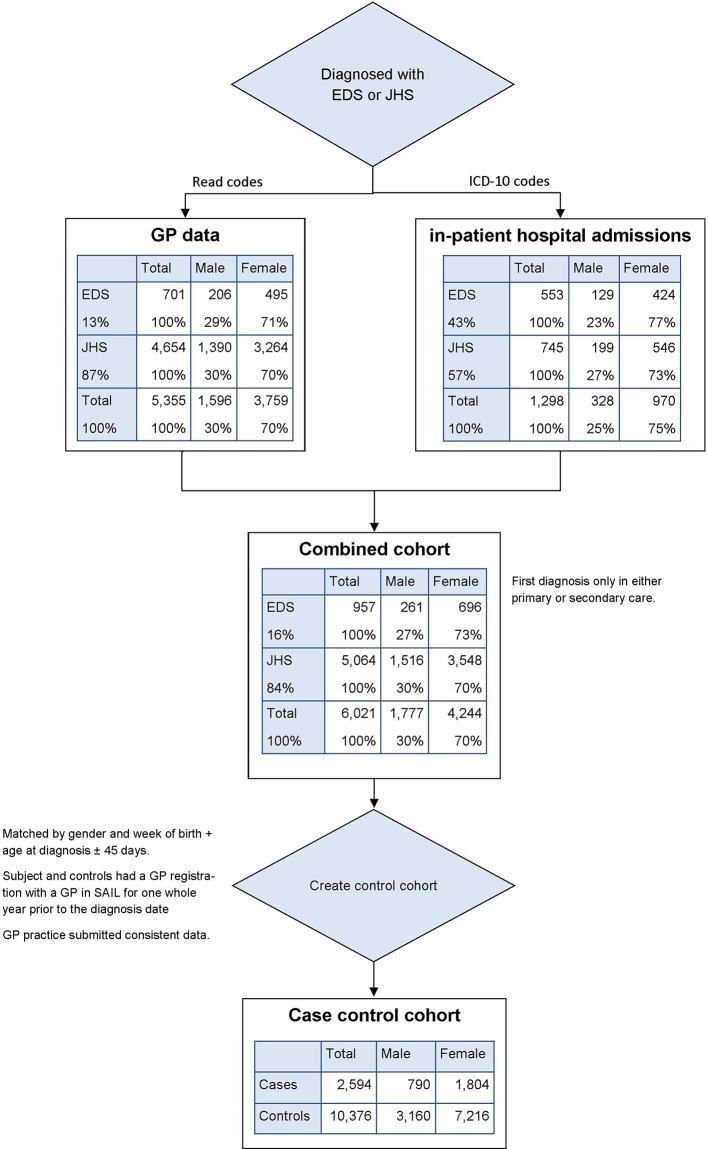
Participants: People within the primary care or hospital data systems with a coded diagnosis of EDS or joint hypermobility syndrome (JHS) between 1 July 1990 and 30 June 2017.
Main outcome measures: Combined prevalence of JHS and EDS in Wales. Additional diagnosis and prescription data in those diagnosed with EDS or JHS compared with matched controls.
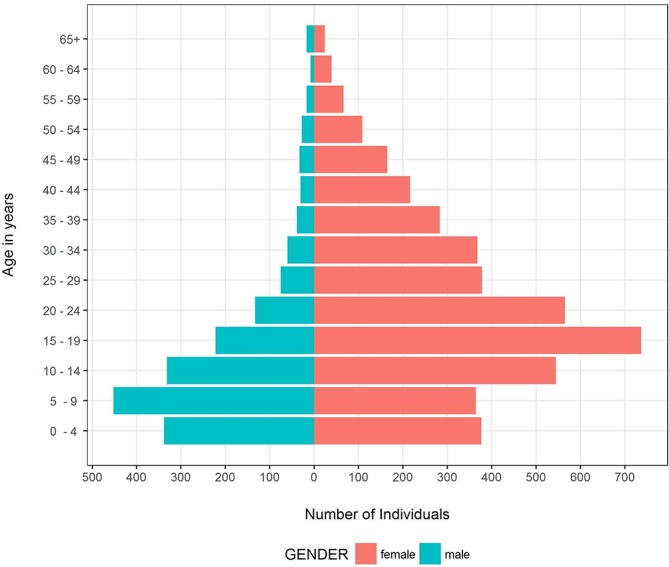
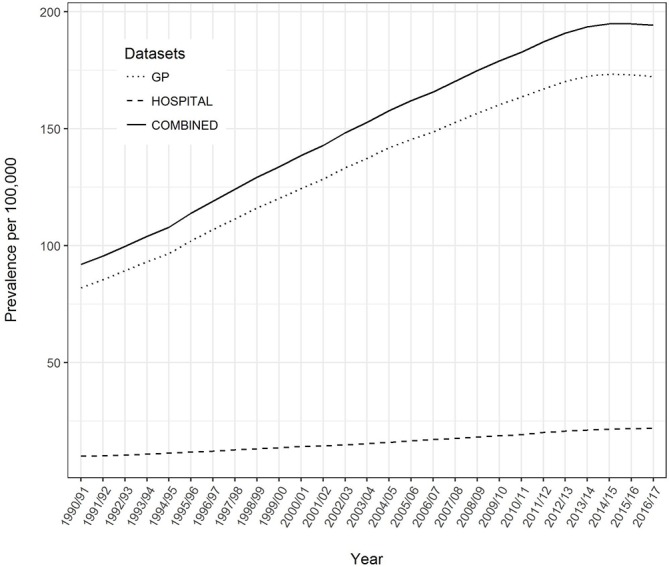
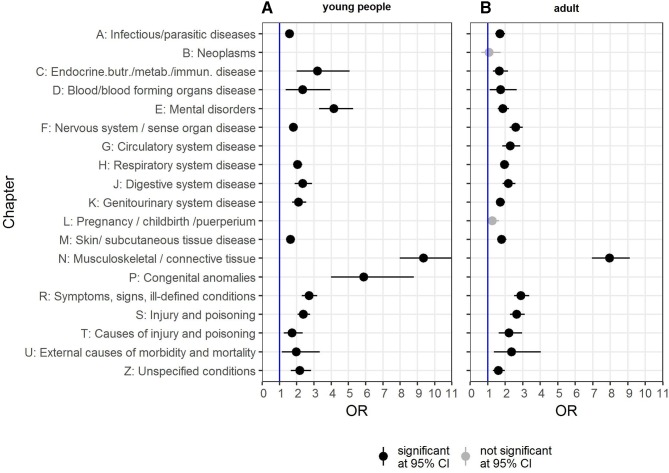
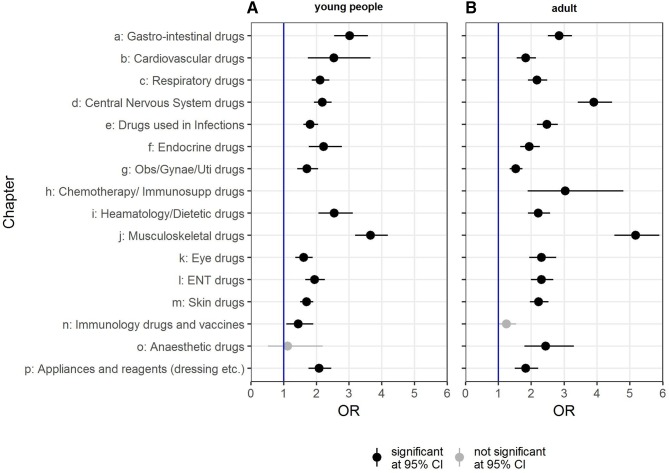
Results: We found 6021 individuals (men: 30%, women: 70%) with a diagnostic code of either EDS or JHS. This gives a diagnosed point prevalence of 194.2 per 100 000 in 2016/2017 or roughly 10 cases in a practice of 5000 patients. There was a pronounced gender difference of 8.5 years (95% CI: 7.70 to 9.22) in the mean age at diagnosis. EDS or JHS was not only associated with high odds for other musculoskeletal diagnoses and drug prescriptions but also with significantly higher odds of a diagnosis in other disease categories (eg, mental health, nervous and digestive systems) and higher odds of a prescription in most disease categories (eg, gastrointestinal and cardiovascular drugs) within the 12 months before and after the first recorded diagnosis.
Conclusions: EDS and JHS (since March 2017 classified as EDS or HSD) have historically been considered rare diseases only affecting the musculoskeletal system and soft tissues. These data demonstrate that both these assertions should be reconsidered.
Keywords: Ehlers-Danlos syndromes; health data linkage; heritable disorders of connective tissue; hypermobility spectrum disorder; joint hypermobility syndrome; prevalence.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Cecil RLF, Goldman L, Bennett JC. Cecil textbook of medicine: W. B. Saunders, 2000.
-
- Commission of the European Communities Commission of the European communities communication from the Commission to the European Parliament, the Council, the European economic and social Committee and the Committee of the regions on rare diseases: Europe's challenges. Brussels: Commission of the European Communities, 2008.
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical