

Thick Graft Versus Double-Bundle Technique on Posterior Cruciate Ligament Reconstruction: Experimental Biomechanical Study with Cadavers
- PMID: 31686711
- PMCID: PMC6819165
- DOI: 10.1016/j.rboe.2017.12.010
Thick Graft Versus Double-Bundle Technique on Posterior Cruciate Ligament Reconstruction: Experimental Biomechanical Study with Cadavers
Abstract
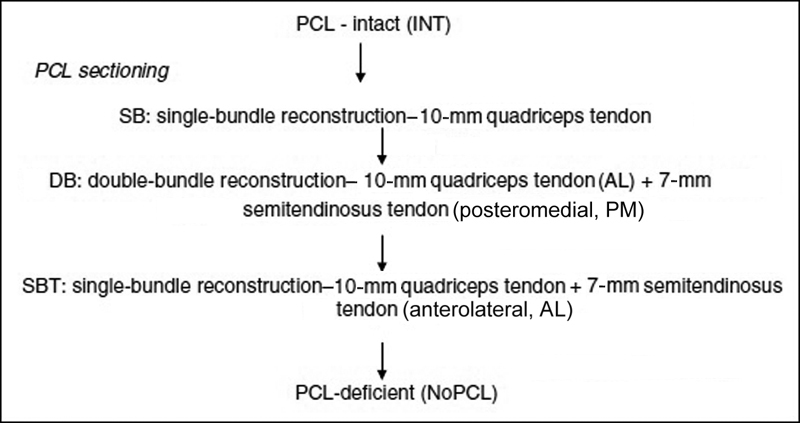
Objective To evaluate the biomechanical effect of graft thickness compared with the double-bundle technique on posterior cruciate ligament (PCL) reconstruction in human cadaveric knees. Methods A total of 9 human cadaveric knees were tested in 5 conditions: intact knee (INT); single-bundle reconstruction with a 10-mm quadriceps tendon (SB); double-bundle reconstruction with a 10 mm-quadriceps tendon for the anterolateral bundle and a 7-mm doubled semitendinosus tendon for the posteromedial bundle (DB); single-bundle reconstruction with a 10-mm quadriceps tendon plus a 7-mm doubled semitendinosus tendon (SBT); and PCL-deficient (NoPCL). The posterior tibial translation (PTT) was measured in response to a 134-N posterior tibial load at 0 ∘ , 30 ∘ , 60 ∘ e 90 ∘ of knee flexion. Results The PTT values of the DB and SBT techniques were always significantly lower (better stability) than those of the SB technique. The PTT values of the SBT technique were significantly lower than those of the DB technique at 60 ∘ ( p = 0.005) and 90 ∘ ( p = 0.001). Conclusions Graft enlargement improves knee stability in isolated PCL reconstructions, whereas the graft division in the two-bundle technique worsens this stability at 60 ∘ and 90 ∘ of knee flexion. The findings of the present study suggest that knee stability in PCL reconstructions may be improved with the use of thicker grafts in the SB technique rather than performing the DB technique.
Keywords: biomechanical phenomena; cadaver; knee injuries; posterior cruciate ligament; posterior cruciate ligament reconstruction.
Conflict of interest statement
Figures







Similar articles
-
Tibial Slope and Its Effect on Graft Force in Posterior Cruciate Ligament Reconstructions.Am J Sports Med. 2019 Apr;47(5):1168-1174. doi: 10.1177/0363546519827958. Epub 2019 Mar 21. Am J Sports Med. 2019. PMID: 30896980
-
Biomechanical Comparison: Single-Bundle versus Double-Bundle Posterior Cruciate Ligament Reconstruction Techniques.J Knee Surg. 2017 May;30(4):347-351. doi: 10.1055/s-0036-1588014. Epub 2016 Aug 20. J Knee Surg. 2017. PMID: 27543681
-
Posterior cruciate ligament graft fixation angles, part 2: biomechanical evaluation for anatomic double-bundle reconstruction.Am J Sports Med. 2014 Oct;42(10):2346-55. doi: 10.1177/0363546514541226. Epub 2014 Aug 4. Am J Sports Med. 2014. PMID: 25091116
-
The role of isolated posterior cruciate ligament reconstruction in knees with combined posterior cruciate ligament and posterolateral complex injury.Knee Surg Sports Traumatol Arthrosc. 2018 Sep;26(9):2669-2678. doi: 10.1007/s00167-017-4672-x. Epub 2017 Aug 14. Knee Surg Sports Traumatol Arthrosc. 2018. PMID: 28808736 Review.
-
Posterior Cruciate Ligament: Current Concepts Review.Arch Bone Jt Surg. 2018 Jan;6(1):8-18. Arch Bone Jt Surg. 2018. PMID: 29430489 Free PMC article. Review.
Cited by
-
Stability of the knee after posterior cruciate ligament reconstruction using peroneus longus tendon graft with three femoral insertion sites. A cadaveric study.Heliyon. 2022 Dec 5;8(12):e11972. doi: 10.1016/j.heliyon.2022.e11972. eCollection 2022 Dec. Heliyon. 2022. PMID: 36506408 Free PMC article.
-
Controversies in acute multiligamentary knee injuries (MLKI).J Exp Orthop. 2020 Jul 27;7(1):56. doi: 10.1186/s40634-020-00260-8. J Exp Orthop. 2020. PMID: 32715370 Free PMC article. Review.
References
-
- Harner C D, Höher J. Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med. 1998;26(03):471–482. - PubMed
-
- Wiley W B, Askew M J, Melby A, III, Noe D A. Kinematics of the posterior cruciate ligament/posterolateral corner-injured knee after reconstruction by single- and double-bundle intra-articular grafts. Am J Sports Med. 2006;34(05):741–748. - PubMed
-
- Kannus P, Bergfeld J, Järvinen M et al.Injuries to the posterior cruciate ligament of the knee. Sports Med. 1991;12(02):110–131. - PubMed
-
- Parolie J M, Bergfeld J A. Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete. Am J Sports Med. 1986;14(01):35–38. - PubMed
-
- Dejour H, Walch G, Peyrot J, Eberhard P. Histoire naturelle de la rupture du ligament croisé postérieur. [The natural history of rupture of the posterior cruciate ligament] Rev Chir Orthop Repar Appar Mot. 1988;74(01):35–43. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous