

Apheresis Therapy for Steroid-Resistant Idiopathic Nephrotic Syndrome: Report on a Case Series
- PMID: 31687235
- PMCID: PMC6803719
- DOI: 10.1155/2019/7304786
Apheresis Therapy for Steroid-Resistant Idiopathic Nephrotic Syndrome: Report on a Case Series
Abstract
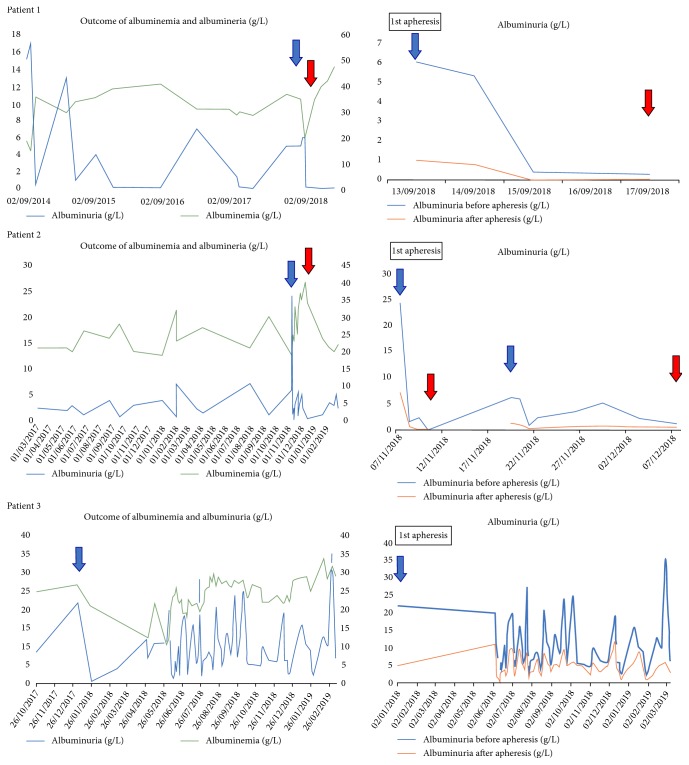
Idiopathic nephrotic syndrome (INS) represents 15%-30% of adulthood glomerulopathies. Corticosteroids have been the main treatment for decades and are effective in 70% of minimal-change disease patients and ~30% of focal segmental glomerulosclerosis patients. Multidrug-resistant (steroids, calcineurin-inhibitors, cyclophosphamide, mycophenolate-mofetil, rituximab) idiopathic nephrotic syndrome is a major therapeutic challenge in nephrology. Apheresis (double-filtration plasmapheresis or semi specific immunoadsorption) could act by eliminating the circulating factor (apolipoproteinA1b, solubleCD40L, suPAR) increasing glomerular permeability seen in INS. The aim of the study was to report the outcome of three patients with multidrug-resistant INS treated successfully with apheresis.
Copyright © 2019 Hamza Naciri Bennani et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
