

Perioperative Acute Kidney Injury
- PMID: 31687986
- PMCID: PMC10924686
- DOI: 10.1097/ALN.0000000000002968
Perioperative Acute Kidney Injury
Abstract
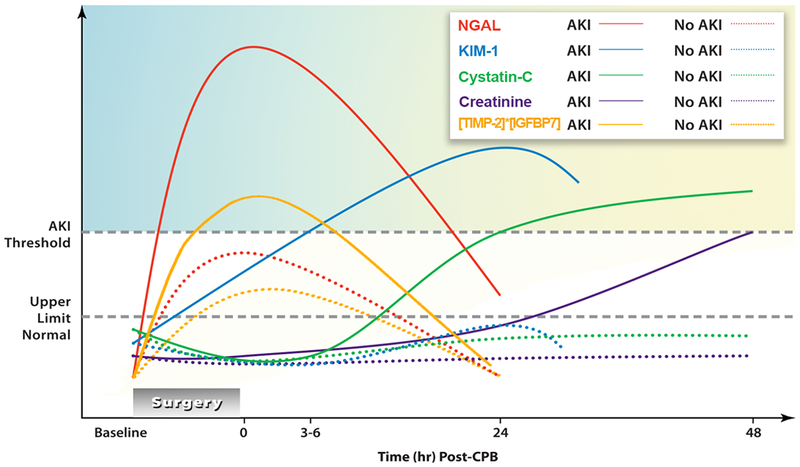
Perioperative organ injury is among the leading causes of morbidity and mortality of surgical patients. Among different types of perioperative organ injury, acute kidney injury occurs particularly frequently and has an exceptionally detrimental effect on surgical outcomes. Currently, acute kidney injury is most commonly diagnosed by assessing increases in serum creatinine concentration or decreased urine output. Recently, novel biomarkers have become a focus of translational research for improving timely detection and prognosis for acute kidney injury. However, specificity and timing of biomarker release continue to present challenges to their integration into existing diagnostic regimens. Despite many clinical trials using various pharmacologic or nonpharmacologic interventions, reliable means to prevent or reverse acute kidney injury are still lacking. Nevertheless, several recent randomized multicenter trials provide new insights into renal replacement strategies, composition of intravenous fluid replacement, goal-directed fluid therapy, or remote ischemic preconditioning in their impact on perioperative acute kidney injury. This review provides an update on the latest progress toward the understanding of disease mechanism, diagnosis, and managing perioperative acute kidney injury, as well as highlights areas of ongoing research efforts for preventing and treating acute kidney injury in surgical patients.
Figures
Comment in
-
Acute Kidney Injury after Surgery: Where Does the Journey Lead?Anesthesiology. 2020 Jan;132(1):5-7. doi: 10.1097/ALN.0000000000003027. Anesthesiology. 2020. PMID: 31687985 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
