

Preoperative Activities of Daily Living Dependency is Associated With Higher 30-Day Readmission Risk for Older Adults After Total Joint Arthroplasty
- PMID: 31688209
- PMCID: PMC7438147
- DOI: 10.1097/CORR.0000000000001040
Preoperative Activities of Daily Living Dependency is Associated With Higher 30-Day Readmission Risk for Older Adults After Total Joint Arthroplasty
Abstract
Background: With recent Medicare payment changes, older adults are increasingly likely to be discharged home instead of to extended care facilities after total joint arthroplasty (TJA), and may therefore be at increased risk for readmissions. Identifying risk factors for readmission could help re-align care pathways for vulnerable patients; recent research has suggested preoperative dependency in activities of daily living (ADL) may increase perioperative and postoperative surgical complications. However, the proportion of older surgical patients with ADL dependence before TJA, and the impact of ADL dependency on the frequency and timing of hospital readmissions is unknown.
Questions/purposes: (1) What proportion of older adults discharged home after TJA have preoperative ADL dependency? (2) Is preoperative ADL dependency associated with increased risk of hospital readmissions at 30 days or 90 days for older adults discharged home after TJA?
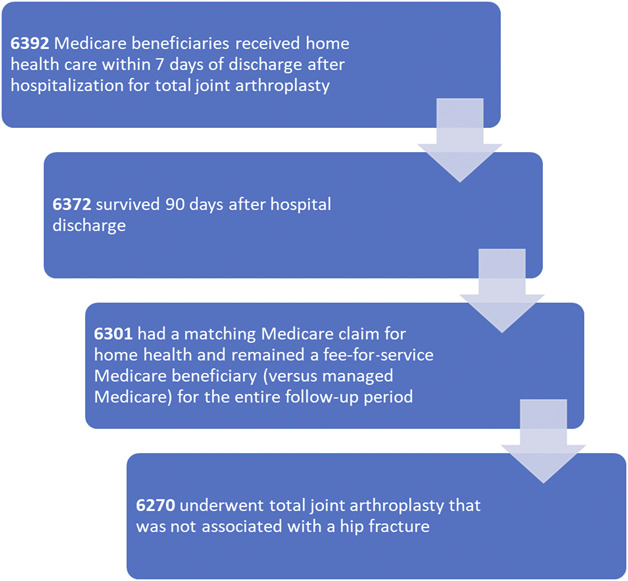
Methods: This was a retrospective cohort analysis of 6270 Medicare fee-for-service claims from 2012 from a 5% national Medicare sample for older adults (older than 65 years) receiving home health care after being discharged to the community after elective TJA. Medicare home health claims were used for two reasons: (1) the primary population of interest was older adults and (2) the accompanying patient-level assessment data included an assessment of prior dependency on four ADL tasks. Activities of daily living dependency was dichotomized as severe (requiring human assistance with all four assessed tasks) or partial/none (needing assistance with three or fewer ADLs); this cutoff has been used in prior research to evaluate readmission risk. Multivariable logistic regression models, clustered at the hospital level and adjusted for known readmission risk factors (such as comorbidity status or age), were used to model the odds of 30- and 90- day and readmission for patients with severe ADL dependence.
Results: Overall, 411 patients were hospitalized during the study period. Of all readmissions, 64% (262 of 411) occurred within the first 30 days, with a median (interquartile range [IQR]) time to readmission of 17 days (5 to 46). Severe ADL dependency before surgery was common for older home health recipients recovering from TJA, affecting 17% (1066 of 6270) of our sample population. After adjusting for clinical covariates, severe ADL dependency was not associated with readmissions at 90 days (adjusted odds ratio = 1.20 [95% CI 0.93 to 1.55]; p = 0.15). However, severe preoperative ADL dependency was associated with higher odds of readmission at 30 days (adjusted OR = 1.45 [95% CI 1.11 to 1.99]; p = 0.008).
Conclusions: Severe preoperative ADL dependency is modestly associated with early but not late hospital readmission after TJA. This work demonstrates that it may important to apply a simple screening of ADL dependency preoperatively so that surgeons can guide changes in care planning for older adults undergoing TJA, which may include participation in preoperative rehabilitation (pre-habilitation) or more aggressive follow-up in the 30 days after surgery. Further research is needed to determine whether severe ADL dependence can be modified before surgery, and whether these changes in dependency can reduce readmission risk after TJA.
Level of evidence: Level III, therapeutic study.
Conflict of interest statement
Each author certifies that neither he or she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: Preoperative Activities of Daily Living Dependency Is Associated With Higher 30-Day Readmission Risk for Older Adults After Total Joint Arthroplasty.Clin Orthop Relat Res. 2020 Feb;478(2):238-240. doi: 10.1097/CORR.0000000000001111. Clin Orthop Relat Res. 2020. PMID: 31899742 Free PMC article. No abstract available.
References
-
- Ayers DC, Fehring TK, Odum SM, Franklin PD. Using joint registry data from FORCE-TJR to improve the accuracy of risk-adjustment prediction models for thirty-day readmission after total hip replacement and total knee replacement. J Bone Joint Surg Am. 2015;97:668-671. - PubMed
-
- Curtis GL, Hammad A, Anis HK, Higuera CA, Little BE, Darwiche HF. Dependent functional status is a risk factor for perioperative and postoperative complications after total hip arthroplasty. J Arthroplasty. 2019;34:S348-S351. - PubMed
-
- Dummit LA, Kahvecioglu D, Marrufo G, Rajkumar R, Marshall J, Tan E, Press MJ, Flood S, Muldoon LD, Gu Q. Association between hospital participation in a Medicare bundled payment initiative and payments and quality outcomes for lower extremity joint replacement episodes. JAMA. 2016;316:1267-1278. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
