

A case report of May-Thurner syndrome induced by anterior lumbar disc herniation: Novel treatment with radiofrequency thermocoagulation
- PMID: 31689801
- PMCID: PMC6946357
- DOI: 10.1097/MD.0000000000017706
A case report of May-Thurner syndrome induced by anterior lumbar disc herniation: Novel treatment with radiofrequency thermocoagulation
Abstract
Rationale: Lumbar degeneration-related May-Thurner syndrome (dMTS) is characterized by venous compression induced by degenerated lower lumbar structures. Treatment strategies for May-Thurner syndrome (MTS) include clearing the thrombus and correcting venous compression. Despite having different etiological factors from other MTS types, treatments for dMTS are similar, including endovascular angioplasty and continuous anticoagulation therapies. Thus, a particular treatment was designed herein to focus on compressive lumbar structures instead of intravenous management.
Patient concerns: A 59-year-old female patient with dMTS, which was induced by inferior vena cava (IVC) stenosis compressed by L4-5 anterior disc herniation.
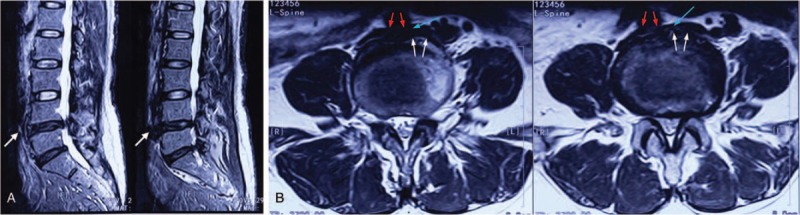
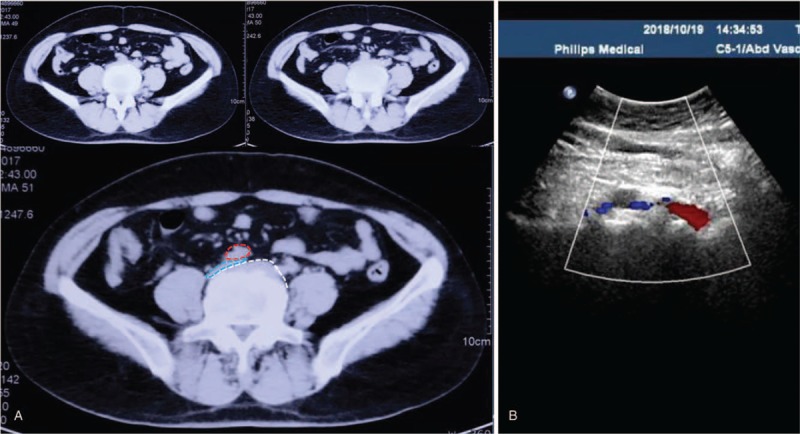
Diagnosis: The patient was diagnosed with IVC stenosis and L4-5 lumbar disc herniation based on abdominal computed tomography, ultrasound, and lumbar magnetic resonance imaging findings.
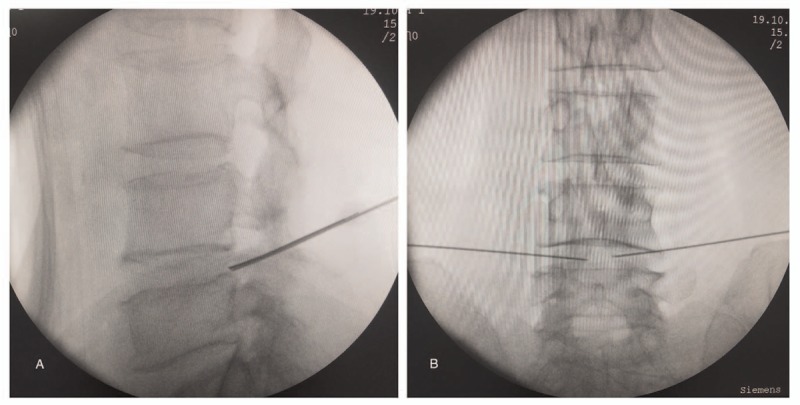
Interventions: Radiofrequency thermocoagulation (RF) was applied to the patient to decrease the compression caused by anterior disc herniation.
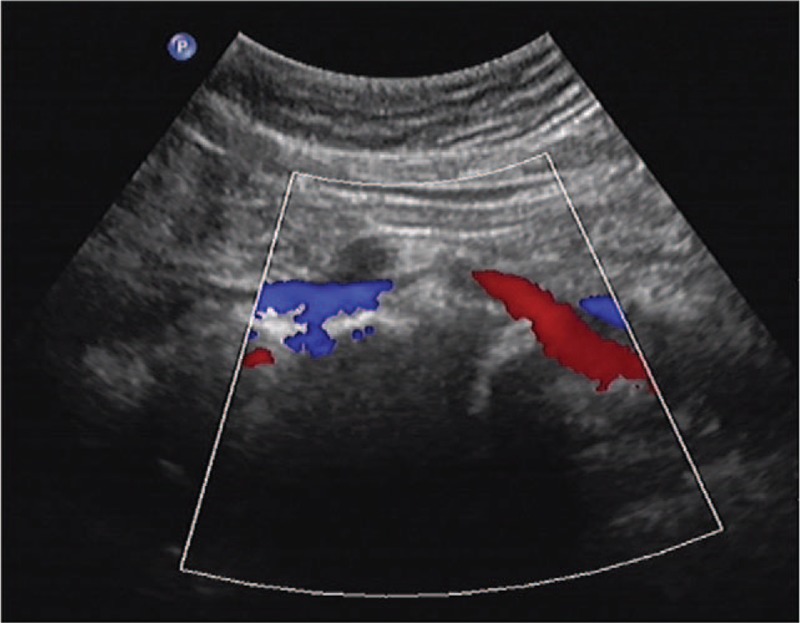
Outcomes: After surgery, the patient's swelling started to improve within 5 hours and completely diminished after 48 hours. Postsurgical abdominal ultrasound showed that her IVC patency increased by 20%. On follow-up, her leg symptoms did not recur at 12 months after surgery.
Lessons: We provided a novel idea in the treatment of dMTS, in which we shifted the treatment focus from endovascular patency restoration to extravascular decompression. Our case proved that RF was effective in treating dMTS, which is a complementary treatment modality to angioplasty.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- May R, Thurner J. The cause of the predominantly sinistral occurrence of thrombosis of the pelvic veins. Angiology 1957;8:419–27. - PubMed
-
- Mousa AY, AbuRahma AF. May-Thurner syndrome: update and review. Ann Vasc Surg 2013;27:984–95. - PubMed
-
- Liddell RP, Evans NS. May-Thurner syndrome. Vasc Med 2018;23:493–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
