

Internet based vestibular rehabilitation with and without physiotherapy support for adults aged 50 and older with a chronic vestibular syndrome in general practice: three armed randomised controlled trial
- PMID: 31690561
- PMCID: PMC6829201
- DOI: 10.1136/bmj.l5922
Internet based vestibular rehabilitation with and without physiotherapy support for adults aged 50 and older with a chronic vestibular syndrome in general practice: three armed randomised controlled trial
Abstract
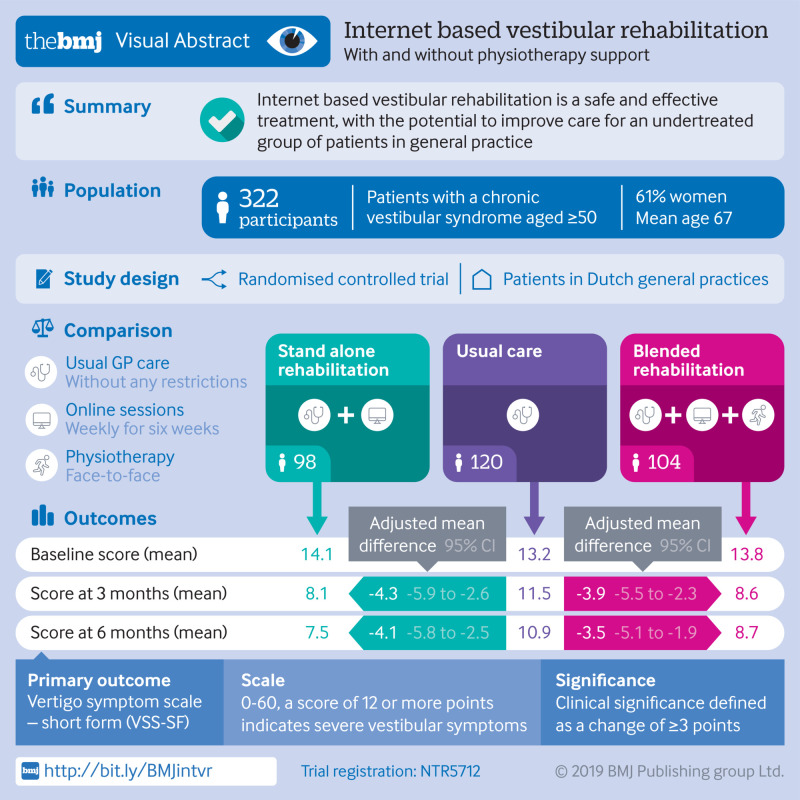
Objective: To investigate the clinical effectiveness and safety of stand alone and blended internet based vestibular rehabilitation (VR) in the management of chronic vestibular syndromes in general practice.
Design: Pragmatic, three armed, parallel group, individually randomised controlled trial.
Setting: 59 general practices in the Netherlands.
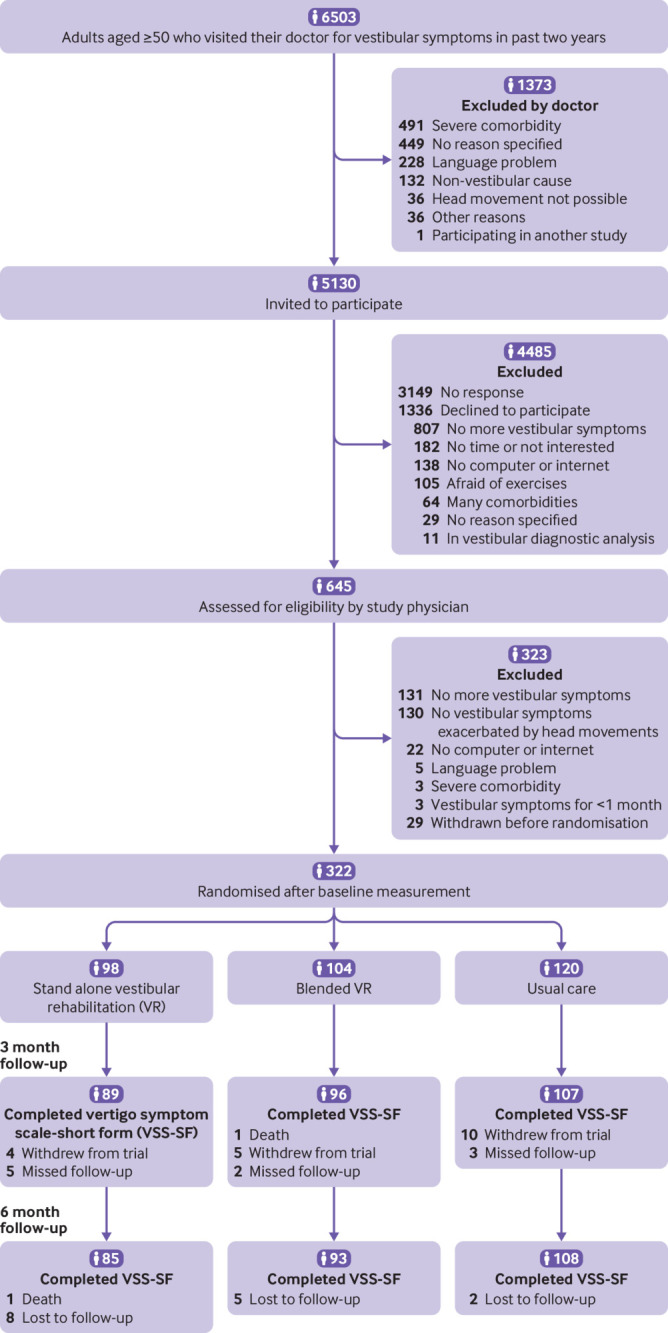
Participants: 322 adults aged 50 and older with a chronic vestibular syndrome.
Interventions: Stand alone VR comprising a six week, internet based intervention with weekly online sessions and daily exercises (10-20 minutes a day). In the blended VR group, the same internet based intervention was supplemented by face-to-face physiotherapy support (home visits in weeks 1 and 3). Participants in the usual care group received standard care from a general practitioner, without any restrictions.
Main outcome measures: The primary outcome was vestibular symptoms after six months as measured by the vertigo symptom scale-short form (VSS-SF range 0-60, clinically relevant difference ≥3 points). Secondary outcomes were dizziness related impairment, anxiety, depressive symptoms, subjective improvement of vestibular symptoms after three and six months, and adverse events.
Results: In the intention-to-treat analysis, participants in the stand alone and blended VR groups had lower VSS-SF scores at six months than participants in the usual care group (adjusted mean difference -4.1 points, 95% confidence interval -5.8 to -2.5; and -3.5 points, -5.1 to -1.9, respectively). Similar differences in VSS-SF scores were seen at three months follow-up. Participants in the stand alone and blended VR groups also experienced less dizziness related impairment, less anxiety, and more subjective improvement of vestibular symptoms at three and six months. No serious adverse events related to online VR occurred during the trial.
Conclusion: Stand alone and blended internet based VR are clinically effective and safe interventions to treat adults aged 50 and older with a chronic vestibular syndrome. Online VR is an easily accessible form of treatment, with the potential to improve care for an undertreated group of patients in general practice.
Trial registration: Netherlands Trial Register NTR5712.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Contributors: ORM obtained the funding and coordinated the study. ORM, VAvV, JCvdW, HEvdH, and LY designed the study. RE and LY advised on the development of the vertigo training intervention. VAvV collected the data. VAvV and JWRT analysed the data. VAvV wrote the first substantial draft of the article and is the guarantor. ORM, JCvdW, RE, LY, HEvdH, and JWRT critically revised the manuscript. All authors read and approved the final manuscript. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the Netherlands Organisation for Health Research and Development (ZonMw) for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
References
-
- Jönsson R, Sixt E, Landahl S, Rosenhall U. Prevalence of dizziness and vertigo in an urban elderly population. J Vestib Res 2004;14:47-52. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical