

Metabolic dysregulation in vitamin E and carnitine shuttle energy mechanisms associate with human frailty
- PMID: 31690722
- PMCID: PMC6831565
- DOI: 10.1038/s41467-019-12716-2
Metabolic dysregulation in vitamin E and carnitine shuttle energy mechanisms associate with human frailty
Abstract
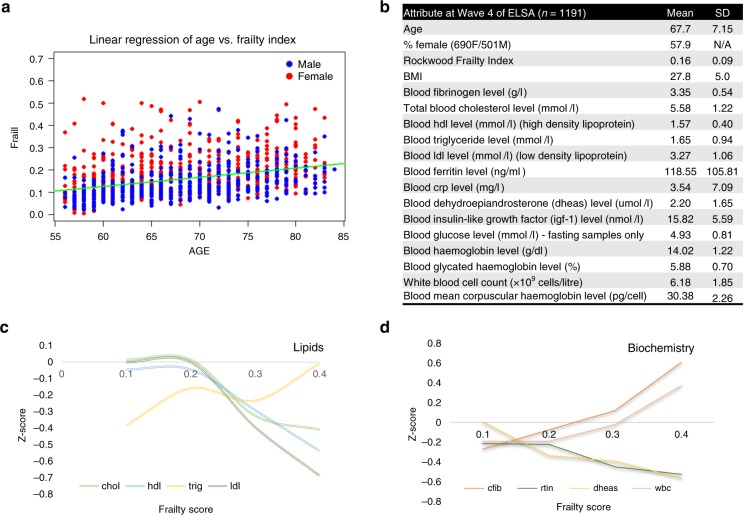
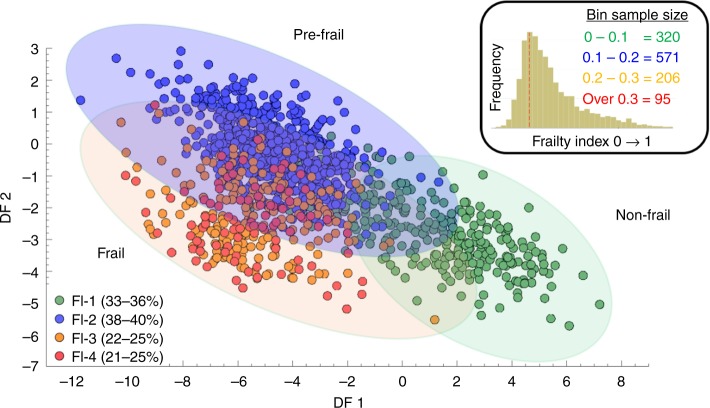
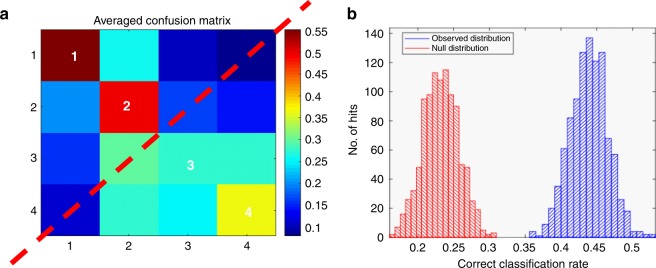
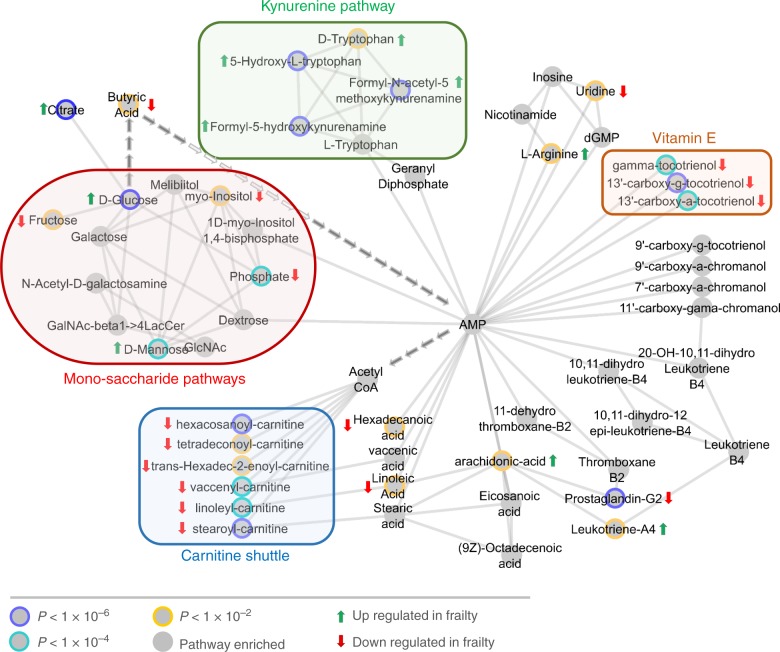
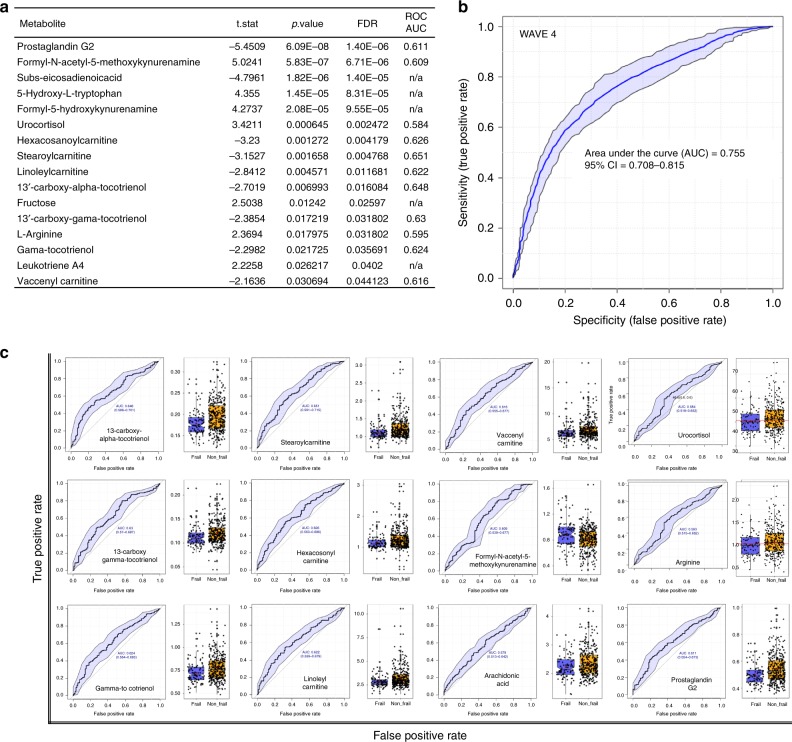
Global ageing poses a substantial economic burden on health and social care costs. Enabling a greater proportion of older people to stay healthy for longer is key to the future sustainability of health, social and economic policy. Frailty and associated decrease in resilience plays a central role in poor health in later life. In this study, we present a population level assessment of the metabolic phenotype associated with frailty. Analysis of serum from 1191 older individuals (aged between 56 and 84 years old) and subsequent longitudinal validation (on 786 subjects) was carried out using liquid and gas chromatography-mass spectrometry metabolomics and stratified across a frailty index designed to quantitatively summarize vulnerability. Through multivariate regression and network modelling and mROC modeling we identified 12 significant metabolites (including three tocotrienols and six carnitines) that differentiate frail and non-frail phenotypes. Our study provides evidence that the dysregulation of carnitine shuttle and vitamin E pathways play a role in the risk of frailty.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- W.H.O. World Health Statistics 2016: Monitoring health for the SDGs (2016).
-
- W.H.O. Ageing and Health Fact Sheet No. 404 (2015).
-
- W.H.O. Global Health and Aging (2017).
-
- Devlin, H. Maximum human lifespan could far exceed 115 years—new research. The Guardian (2017).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
