

Myofascial trigger points alter the modular control during the execution of a reaching task: a pilot study
- PMID: 31690799
- PMCID: PMC6831581
- DOI: 10.1038/s41598-019-52561-3
Myofascial trigger points alter the modular control during the execution of a reaching task: a pilot study
Abstract
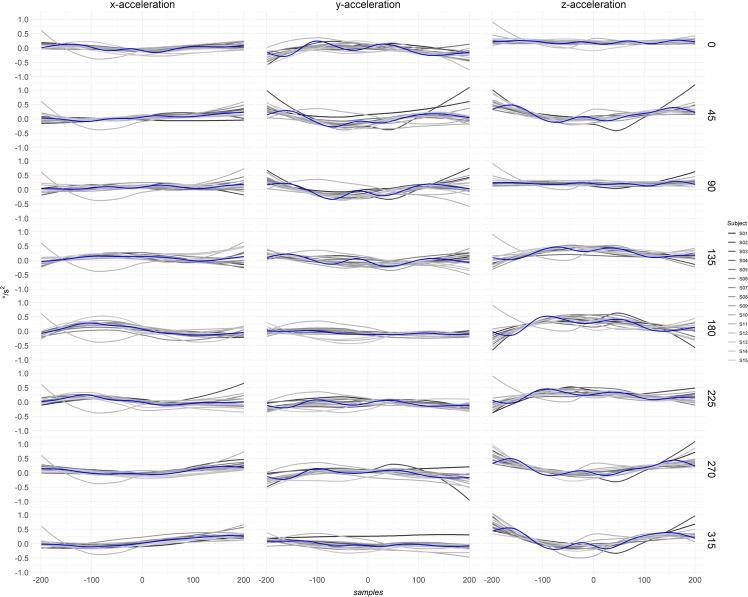
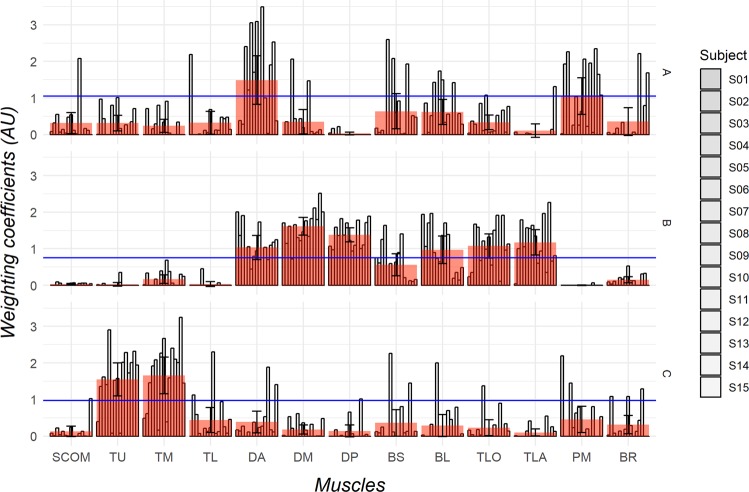
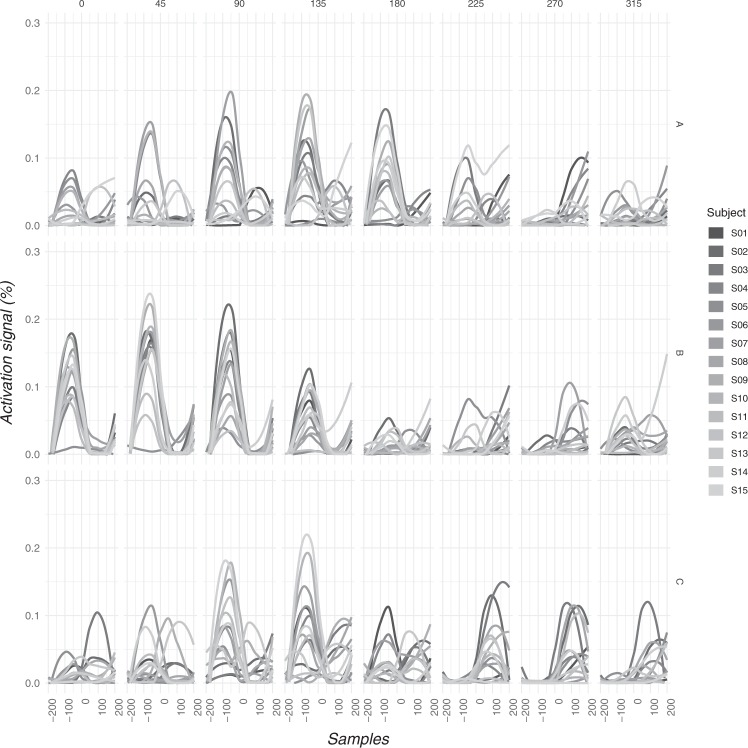
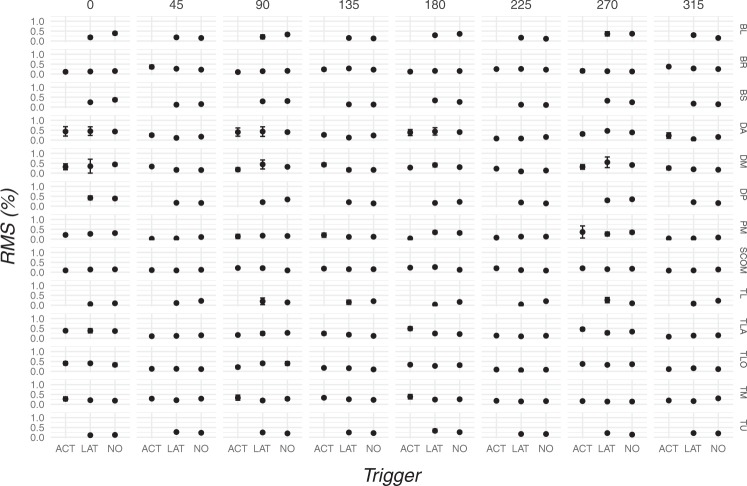
Myofascial trigger points (TP) constitute a conundrum in research and clinical practice as their etiopathogenesis is debated. Several studies investigating one or few muscles have shown that both active and latent TP causes an increased muscle activity, however the influence of TP on modular motor control during a reaching task is still unclear. Electromyographic signals, recorded from the muscles of the shoulder girdle and upper arm during a reaching task, were decomposed with Non-Negative Matrix Factorization algorithm. The extracted matrices of motor modules and activation signals were used to label the muscles condition as dominant or non-dominant. The presence of latent and active TP was detected in each muscle with manual examination. Despite a similar muscle activity was observed, we found that muscles with active TP had increased weighting coefficients when labeled in the dominant condition. No influences were found when muscles were in the non-dominant condition. These findings suggest that TP altered the motor control without co-contraction patterns. As a preliminary evidence, the present results suggest that the increased weighting coefficients in presence of TPs are associated with an alteration of the modular motor control without affecting the dimensionality of motor modules for each individual and reciprocal inhibition.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Simons, D. G., Travell, J. G. & Simons, L. S. Myofascial pain and dysfunction. The trigger point manual. 2nd edn Vol.1 Upper half of the body. (Williams & Wilkins, 1999).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
