

The predictive value of cervical shear wave elastography in the outcome of labor induction
- PMID: 31691266
- PMCID: PMC6973099
- DOI: 10.1111/aogs.13706
The predictive value of cervical shear wave elastography in the outcome of labor induction
Abstract
Introduction: Bishop score, the traditional method to assess cervical condition, is not a promising predictive tool of the outcome of labor induction. As an objective assessment tool, many cervical ultrasound measurements have been proposed to represent the individual components of the Bishop score, but none of them can measure the cervical stiffness. Cervical shear wave elastography is a novel tool to assess the cervical stiffness quantitatively.
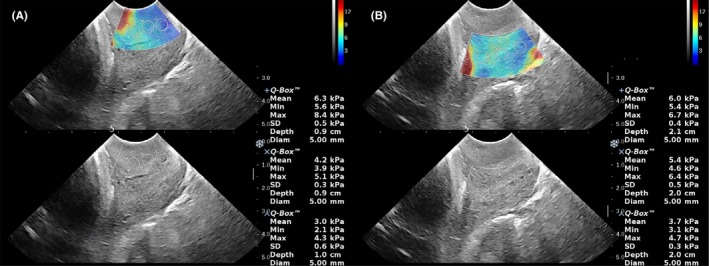
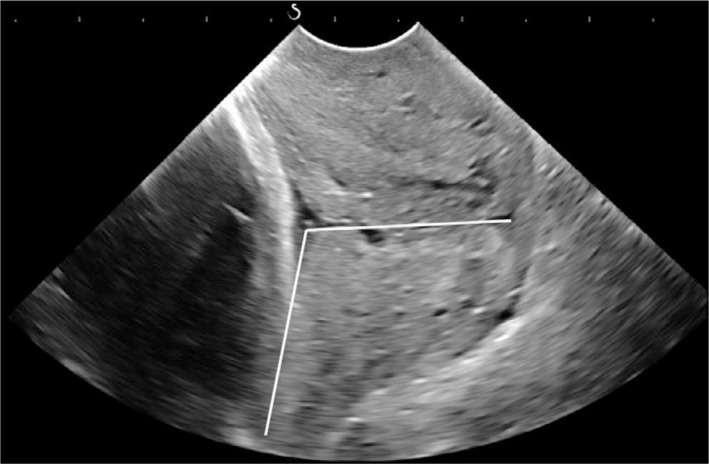
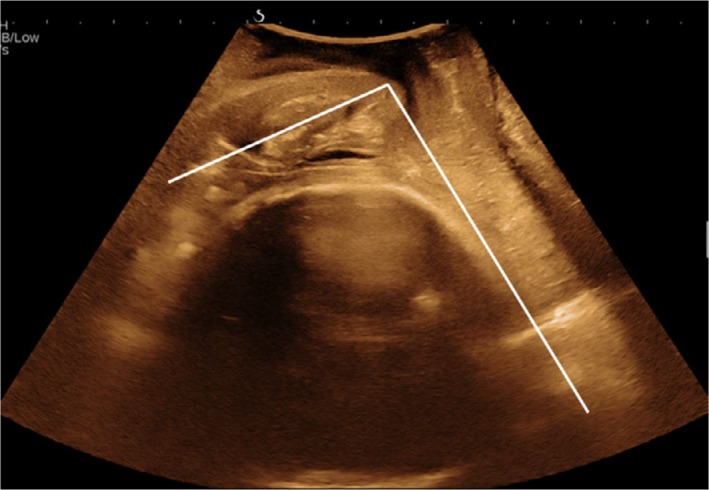
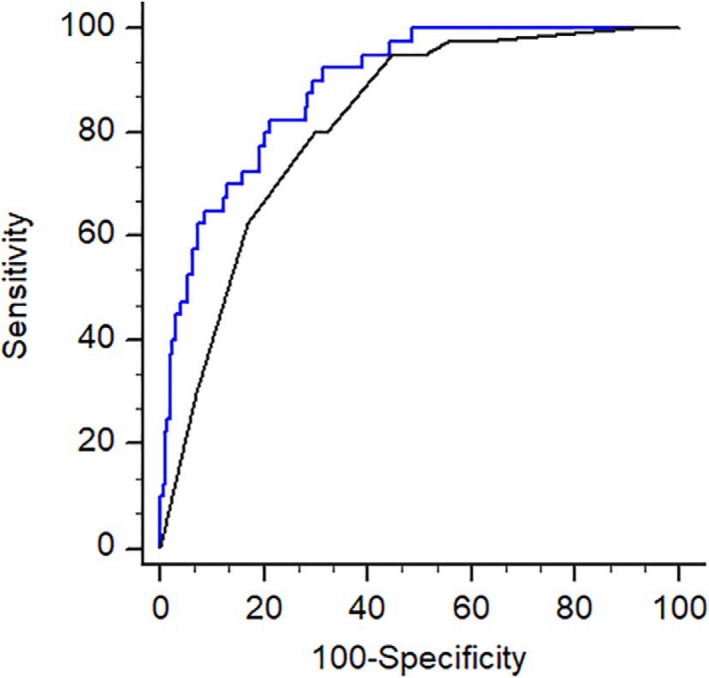
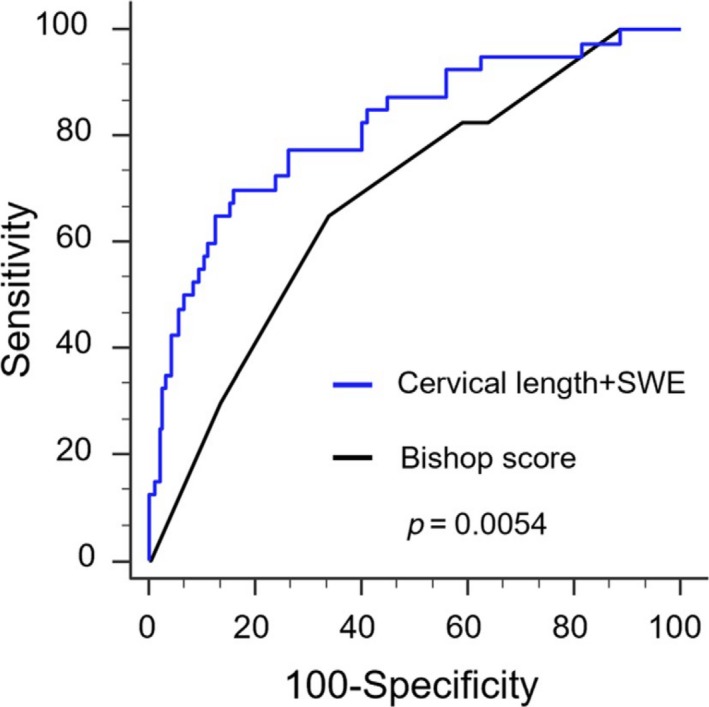
Material and methods: A total of 475 women who required labor induction were studied prospectively. Prior to routine digital assessment of the Bishop score, transvaginal sonographic measurement of cervical length, posterior cervical angle, angle of progression and shear wave elastography was performed. Shear wave elastography measurement was made at the inner, middle and outer regions of the cervix to assess homogeneity. Association of labor induction outcomes including the overall cesarean section and subgroups of cesarean section for failure to enter active phase, with cervical sonographic parameters and the Bishop score, were assessed using multivariate regression analyses. The predictive accuracy of the outcomes using models based on ultrasound measurement and the Bishop score was compared using the area under the receiver-operating characteristics curves.
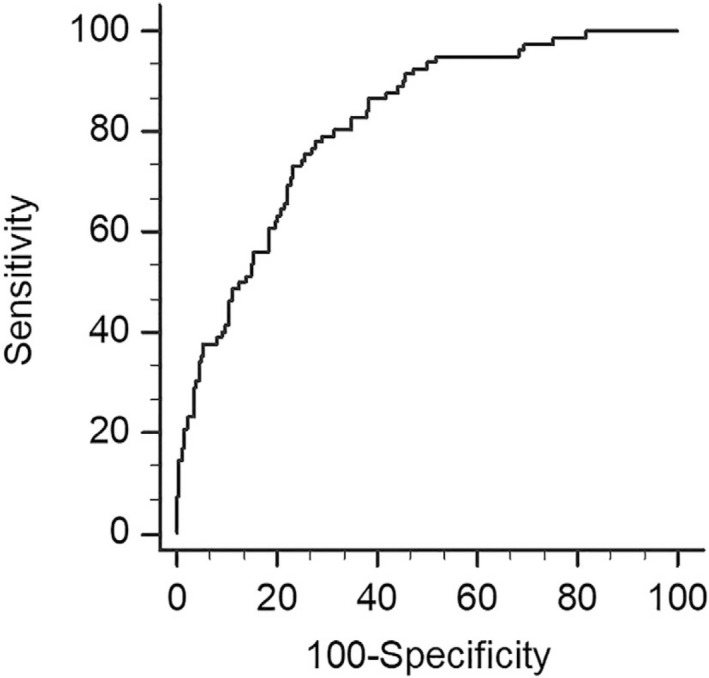
Results: Among 475 women, 82 (17.3%) required cesarean section. Shear wave elasticity was significantly higher in the inner cervical region than in other regions, indicating a greater stiffness (P < 0.001). Both inner cervical shear wave elasticity and cervical length were independent predictors of overall cesarean section (respective adjusted odds ratio [95% CI] 1.338 [1.001-1.598] and 1.717 [1.077-1.663]) and cesarean section for failure to enter active phase (respective adjusted odds ratio [95% CI] 1.689 [1.234-2.311] and 2.556 [1.462-4.467]), after adjusting for other covariates. Outcome prediction models using inner cervical shear wave elasticity and cervical length, had increased area under curve compared with models using the Bishop score (0.888 vs 0.819, P = 0.009).
Conclusions: The cervix is not a homogenous structure, with the inner cervix having the highest stiffness, which is an independent predictor of overall cesarean section, and specifically for those indicated because of failure to enter active phase. Models based on shear wave elastography and cervical length had higher predictive accuracy than models based on the Bishop score.
Keywords: Bishop score; angle of progression; cervical length; induction of labor; posterior cervical angle; prediction; shear wave elastography.
© 2019 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Figures
References
-
- Rayburn WF, Zhang J. Riding rates of labor induction: present concerns and future strategies. Obstet Gynecol. 2002;100:164‐167. - PubMed
-
- Bishop EH. Pelvic scoring for elective induction. Obstet Gynecol. 1964;24:266‐268. - PubMed
-
- Faltin‐traub EF, Boulvain M, Faltin DL, Extermann P, Irion O. Reliability of the Bishop score before labour induction at term. Eur J Obstet Gynaecol Reprod Biol. 2004;112:178‐181. - PubMed
-
- Kolkman DG, Verhoeven CJ, Brinkhorst SJ, et al. The Bishop score as a predictor of labor induction success: a systematic review. Am J Perinatol. 2013;30:625‐630. - PubMed
-
- Rane SM, Guirgis RR, Higgins B, Nicolaides KH. The value of ultrasound in the prediction of successful induction of labor. Ultrasound Obstet Gynecol. 2004;24:538‐549. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
