

Comorbidity in trichotillomania (hair-pulling disorder): A cluster analytical approach
- PMID: 31692297
- PMCID: PMC6908854
- DOI: 10.1002/brb3.1456
Comorbidity in trichotillomania (hair-pulling disorder): A cluster analytical approach
Abstract
Background: A promising approach to reducing the phenotypic heterogeneity of psychiatric disorders involves the identification of homogeneous subtypes. Careful study of comorbidity in obsessive-compulsive disorder (OCD) contributed to the identification of the DSM-5 subtype of OCD with tics. Here we investigated one of the largest available cohorts of clinically diagnosed trichotillomania (TTM) to determine whether subtyping TTM based on comorbidity would help delineate clinically meaningful subgroups.
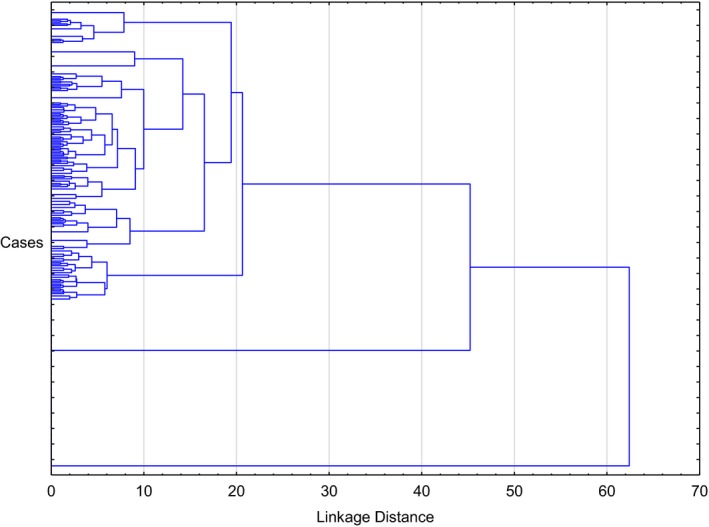
Methods: As part of an ongoing international collaboration, lifetime comorbidity data were collated from 304 adults with pathological hair-pulling who fulfilled criteria for DSM-IV-TR or DSM-5 TTM. Cluster analysis (Ward's method) based on comorbidities was undertaken.
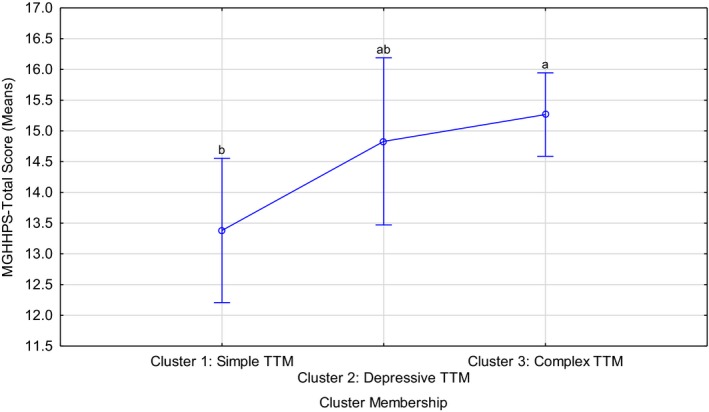
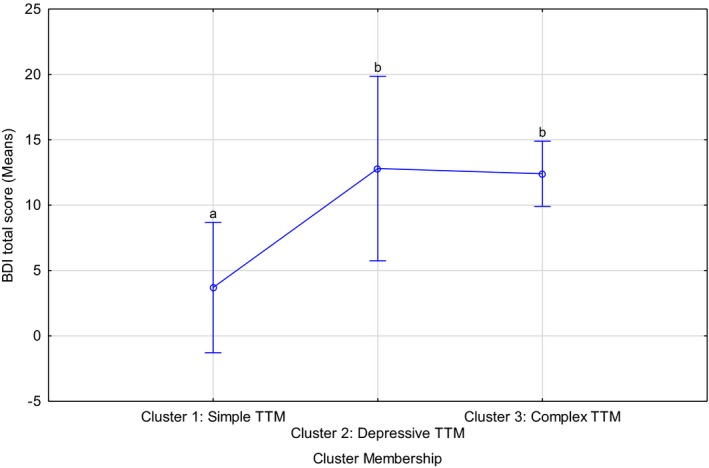
Results: Three clusters were identified, namely Cluster 1: cases without any comorbidities (n = 63, 20.7%) labeled "simple TTM," Cluster 2: cases with comorbid major depressive disorder only (N = 49, 16.12%) labeled "depressive TTM," and Cluster 3: cases presenting with combinations of the investigated comorbidities (N = 192, 63.16%) labeled "complex TTM." The clusters differed in terms of hair-pulling severity (F = 3.75, p = .02; Kruskal-Wallis [KW] p < .01) and depression symptom severity (F = 5.07, p = <.01; KW p < .01), with cases with any comorbidity presenting with increased severity. Analysis of the temporal nature of these conditions in a subset suggested that TTM onset generally preceded major depressive disorder in (subsets of) Clusters 2 and 3.
Conclusions: The findings here are useful in emphasizing that while many TTM patients present without comorbidity, depression is present in a substantial proportion of cases. In clinical practice, it is crucial to assess comorbidity, given the links demonstrated here between comorbidity and symptom severity. Additional research is needed to replicate these findings and to determine whether cluster membership based on comorbidity predicts response to treatment.
Keywords: borderline personality disorder; comorbidity; depression; treatment; trichotillomania.
© 2019 The Authors. Brain and Behavior published by Wiley Periodicals, Inc.
Conflict of interest statement
None declared.
Figures
References
-
- American Psychiatric Association (2000). American Psychiatric Association diagnostic and statistical manual of mental disorders 4th edition – Text revision (DSM‐IV‐TR). Washington, DC: American Psychiatric Association.
-
- American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (DSM‐5). Arlington, VA: American Psychiatric Publishing.
-
- Beck, A. T. , Steer, R. A. , & Garbin, M. G. (1988). Psychometric properties of the beck depression inventory – 25 years of evaluation. Clinical Psychology Review, 8, 77–100.
-
- Beck, A. T. , Ward, C. H. , Mendelson, M. , Mock, J. , & Erbaugh, J. (1961). An inventory for measuring depression. Archives of General Psychiatry, 4, 561–571. - PubMed
-
- Diefenbach, G. J. , Tolin, D. F. , Crocetto, J. , Maltby, N. , & Hannan, S. (2005). Assessment of Trichotillomania: A psychometric evaluation of hair‐pulling scales. Journal of Psychopathology and Behavioral Assessment, 27(2), 169–178.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
