

Coronary CT radiation dose reduction strategies at an Australian Tertiary Care Center - improvements in radiation exposure through an evidence-based approach
- PMID: 31693313
- PMCID: PMC7063243
- DOI: 10.1002/jmrs.358
Coronary CT radiation dose reduction strategies at an Australian Tertiary Care Center - improvements in radiation exposure through an evidence-based approach
Abstract
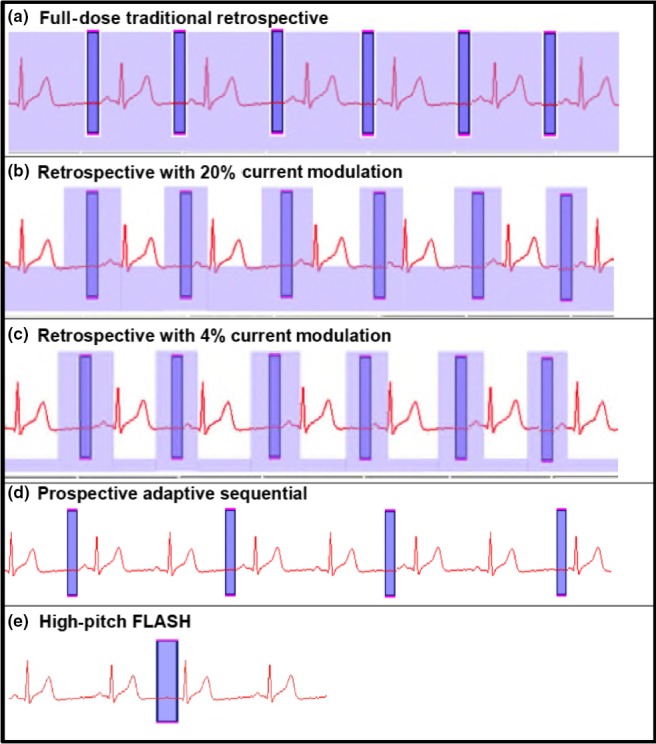
Introduction: Coronary CT Angiography (CCTA) is a rapidly increasing technique for coronary imaging; however, it exposes patients to ionising radiation. We examined the impact of dose reduction techniques using ECG-triggering, kVp/mAs reduction and high-pitch modes on radiation exposure in a large Australian tertiary CCTA service.
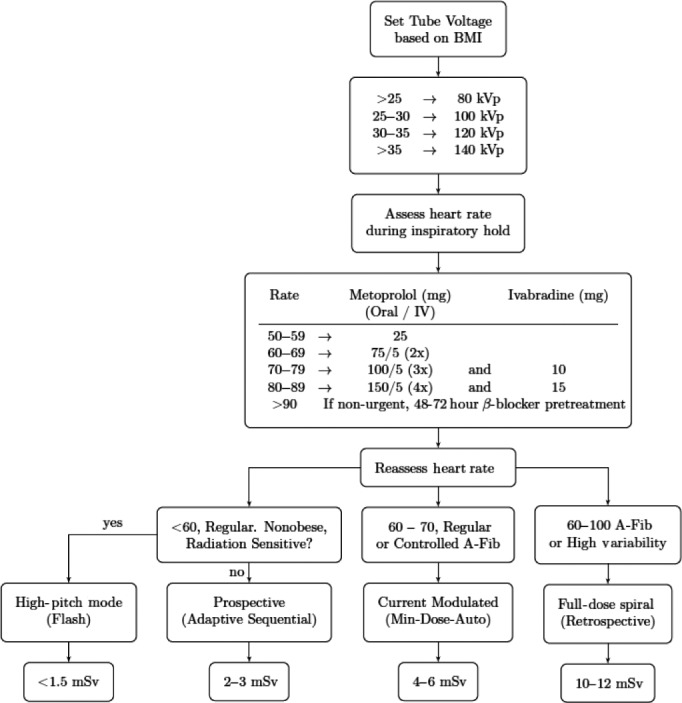
Methods: Data on acquisition modes and dose exposure were prospectively collected on all CCTA scans from November 2009 to March 2014 at an Australian tertiary care centre. A dose reduction algorithm was developed using published techniques and implemented with education of medical staff, radiographers and referrers. Associations of CCTA acquisition to radiation over time were analysed with multivariate regression. Specificity in positive CCTA was assessed by correlation with invasive coronary angiography.
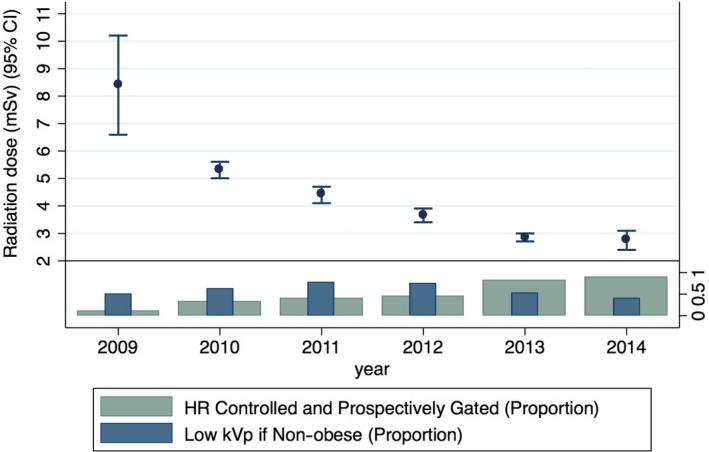
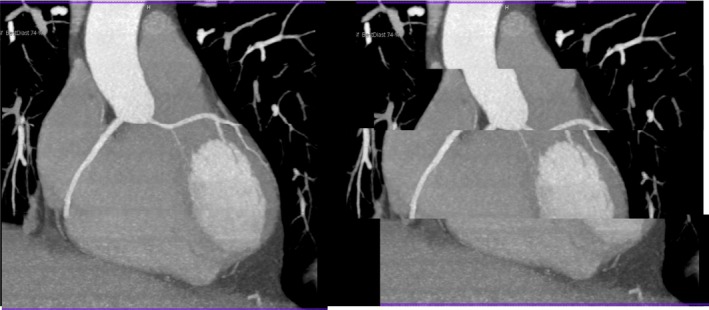
Results: 3333 CCTAs were analysed. Mean radiation dose decreased from 8.4 mSv to 5.3, 4.4, 3.7, 2.9 and 2.8 mSv (P < 0.001) per year. Patient characteristics were unchanged. Dose reduction strategies using ECG-triggering, kVp/mAs reduction accounted for 91% of the decrease. High-pitch scanning reduced dose by an additional 9%. Lower dose was independently related to lower kVp, heart rate, tube current modulation, BMI, prospective triggering and high-pitch mode (P < 0.01). CCTA specificity remained unchanged despite dose reduction.
Conclusion: Implementation of evidence-based CCTA dose reduction algorithm and staff education programme resulted in a 67% reduction in radiation exposure, while maintaining diagnostic specificity. This approach is widely applicable to clinical practice for the performance of CCTA.
Keywords: cardiovascular computed tomography; coronary CT; education; prospectively triggered coronary CT; radiation dose; tube voltage.
© 2019 The Authors and State of Queensland Journal of Medical Radiation Sciences published by John Wiley & Sons Australia, Ltd on behalf of Australian Society of Medical Imaging and Radiation Therapy and New Zealand Institute of Medical Radiation Technology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Taylor AJ, Cerqueira M, Hodgson JM, et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J Am Coll Cardiol 2010; 56: 1864–94. - PubMed
-
- Raff GL. Radiation dose from coronary CT angiography: five years of progress. J Cardiovasc Comput Tomogr 2010; 4: 365–74. - PubMed
-
- Bischoff B, Hein F, Meyer T, et al. Comparison of sequential and helical scanning for radiation dose and image quality: results of the Prospective Multicenter Study on Radiation Dose Estimates of Cardiac CT Angiography (PROTECTION) I Study. AJR Am J Roentgenol 2010; 194: 1495–9. - PubMed
-
- Hausleiter J, Martinoff S, Hadamitzky M, et al. Image quality and radiation exposure with a low tube voltage protocol for coronary CT angiography results of the PROTECTION II Trial. JACC Cardiovasc Imaging 2010; 3: 1113–23. - PubMed
-
- Hausleiter J, Meyer TS, Martuscelli E, et al. Image quality and radiation exposure with prospectively ECG‐triggered axial scanning for coronary CT angiography: the multicenter, multivendor, randomized PROTECTION‐III study. JACC Cardiovasc Imaging 2012; 5: 484–93. - PubMed
