

Subclinical and Device-Detected Atrial Fibrillation: Pondering the Knowledge Gap: A Scientific Statement From the American Heart Association
- PMID: 31694402
- PMCID: PMC8438789
- DOI: 10.1161/CIR.0000000000000740
Subclinical and Device-Detected Atrial Fibrillation: Pondering the Knowledge Gap: A Scientific Statement From the American Heart Association
Abstract
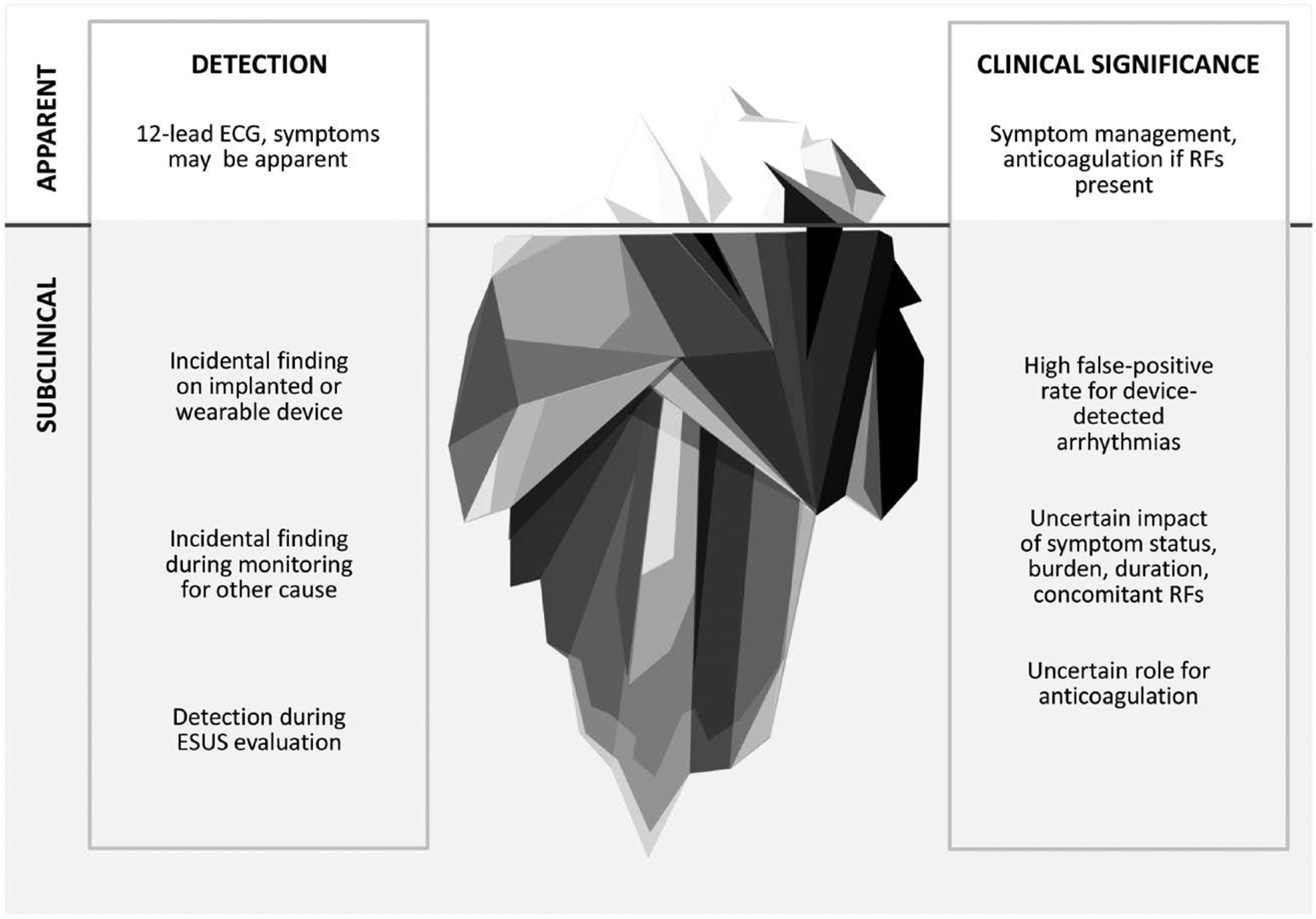
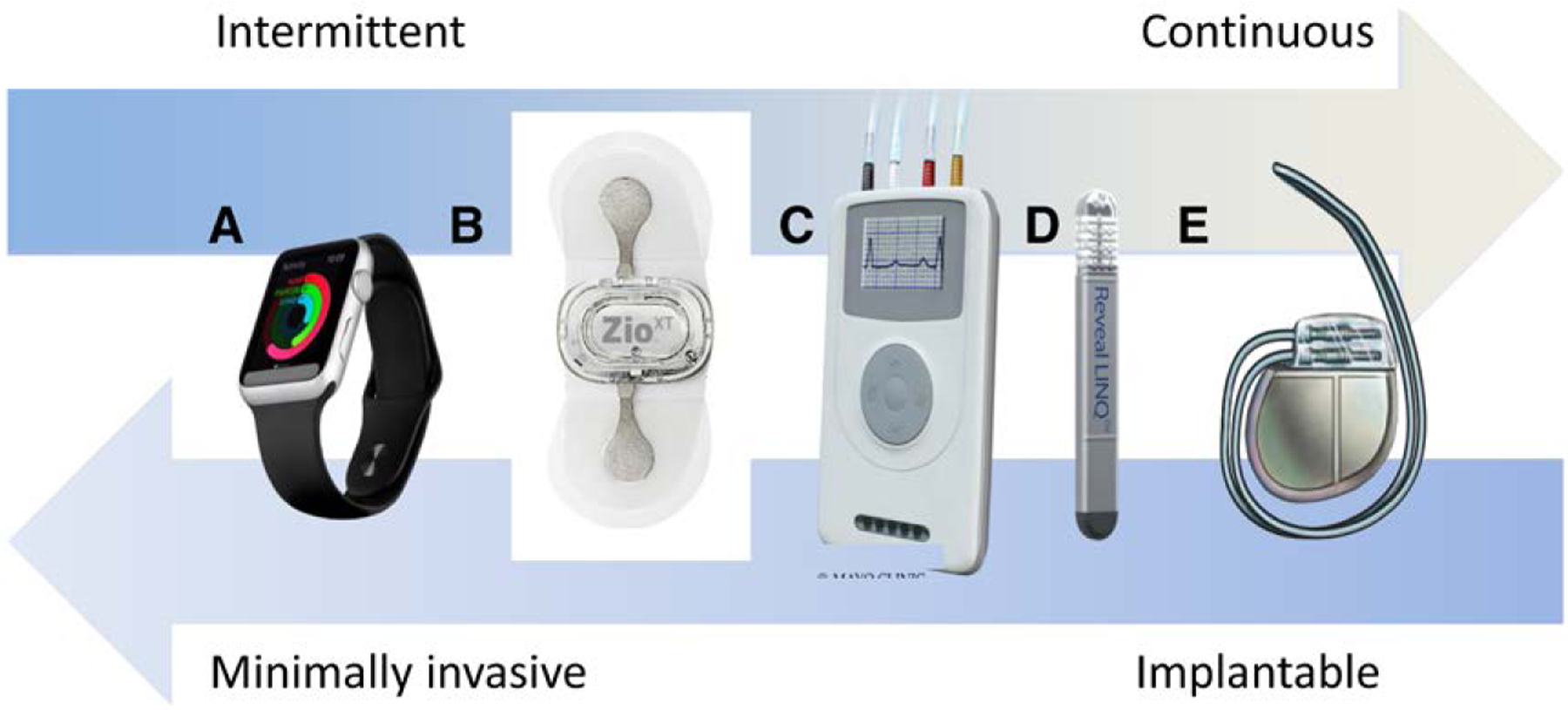
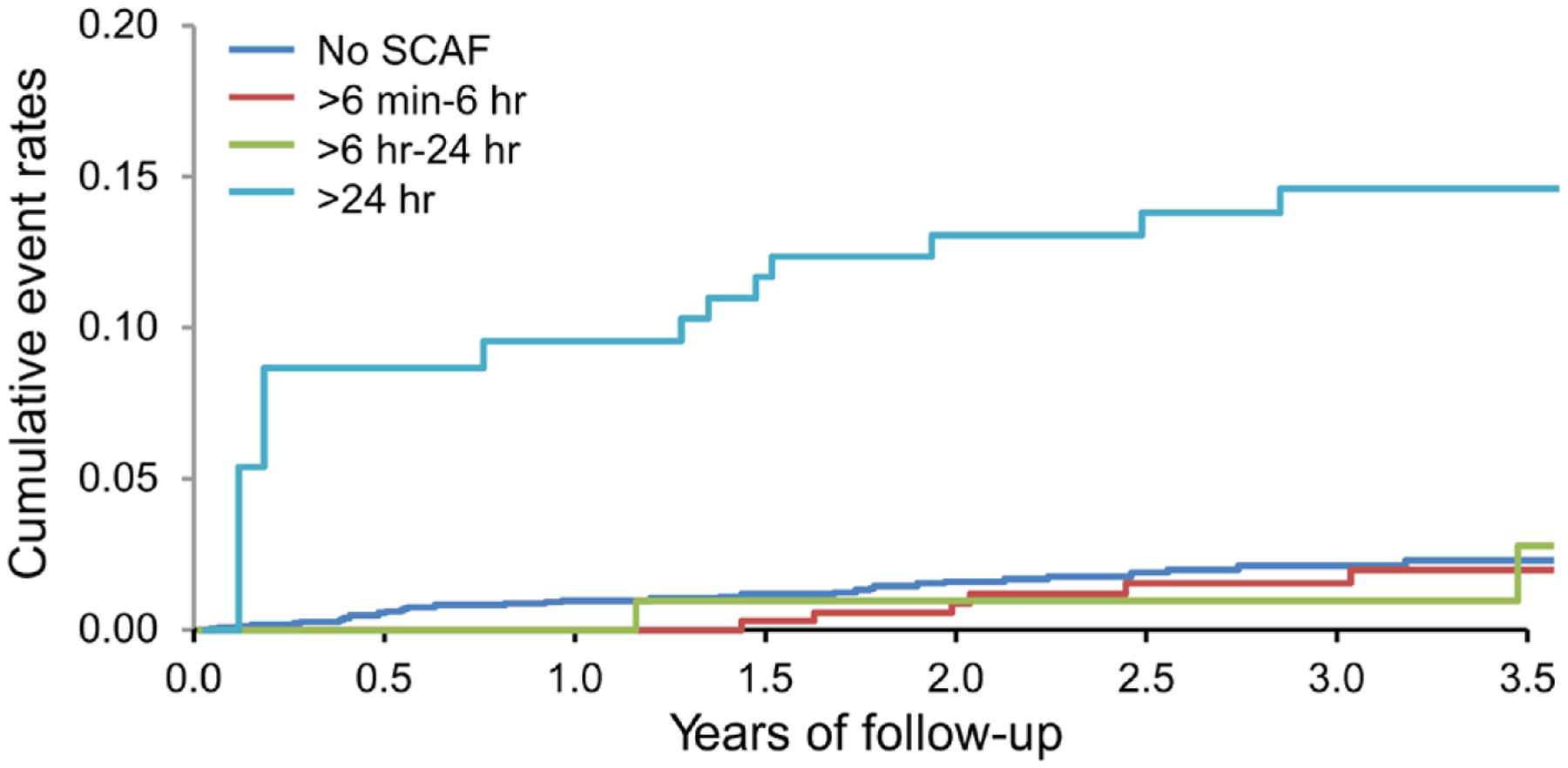
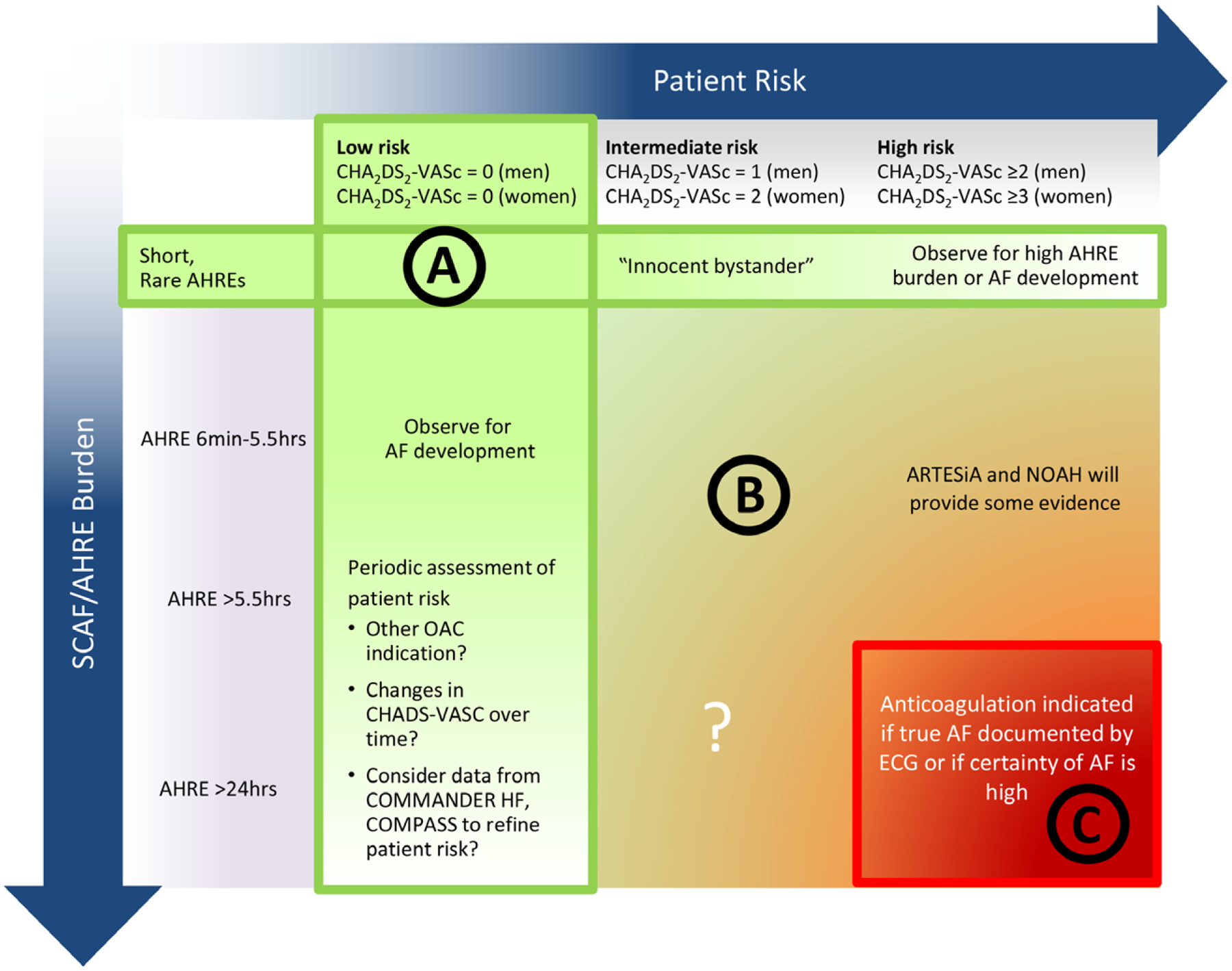
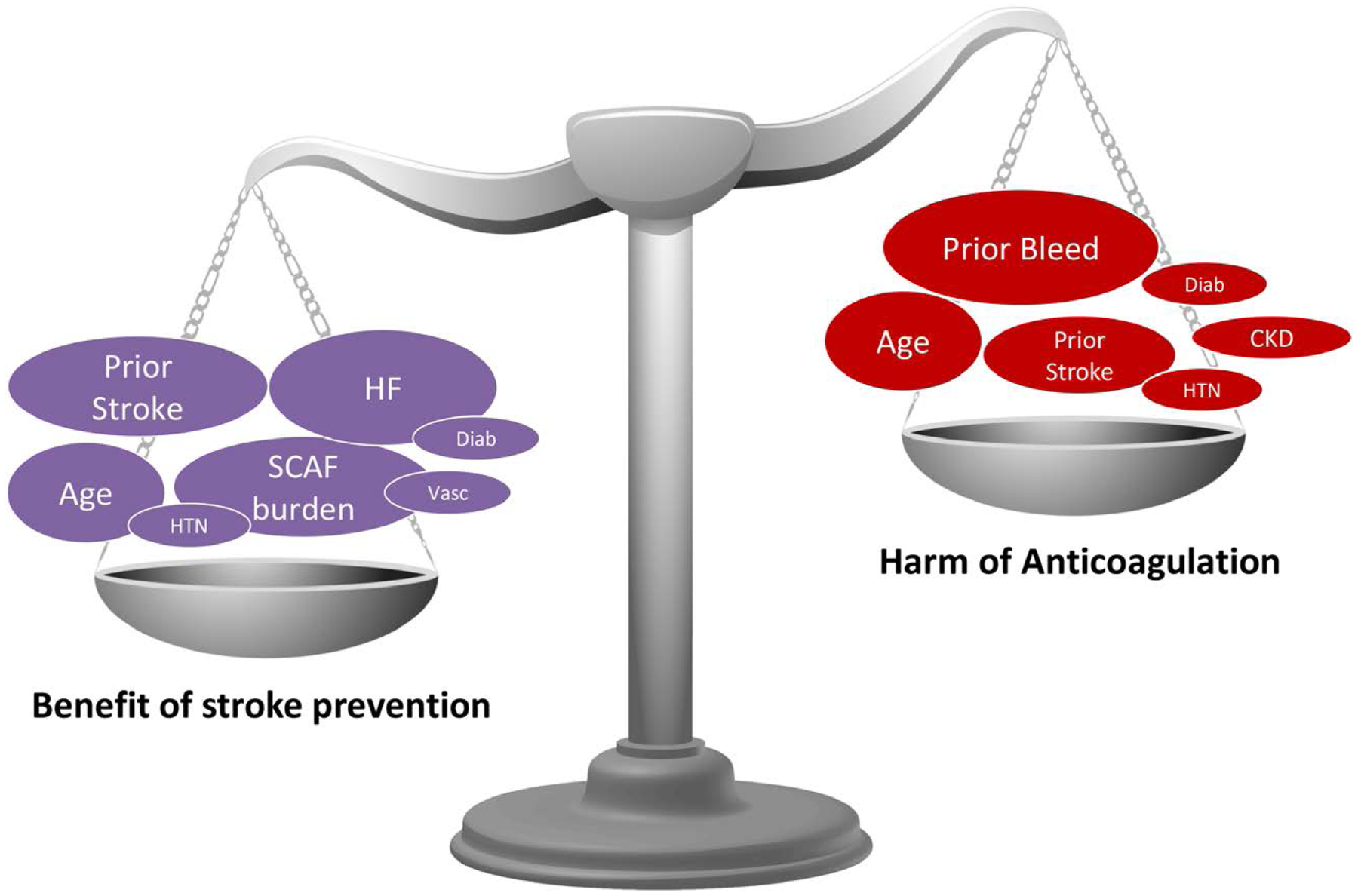
The widespread use of cardiac implantable electronic devices and wearable monitors has led to the detection of subclinical atrial fibrillation in a substantial proportion of patients. There is evidence that these asymptomatic arrhythmias are associated with increased risk of stroke. Thus, detection of subclinical atrial fibrillation may offer an opportunity to reduce stroke risk by initiating anticoagulation. However, it is unknown whether long-term anticoagulation is warranted and in what populations. This scientific statement explores the existing data on the prevalence, clinical significance, and management of subclinical atrial fibrillation and identifies current gaps in knowledge and areas of controversy and consensus.
Keywords: AHA Scientific Statements; ambulatory monitoring; atrial fibrillation; cardiac arrhythmia; cardiac pacing; cerebrovascular stroke; pacemaker.
Conflict of interest statement
The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
Figures
Comment in
-
Device-Detected Subclinical Atrial Fibrillation: The Anesthesiologist's Perspective.J Cardiothorac Vasc Anesth. 2020 Nov;34(11):2876-2880. doi: 10.1053/j.jvca.2020.05.036. Epub 2020 Jun 4. J Cardiothorac Vasc Anesth. 2020. PMID: 32690237 No abstract available.
References
-
- Noseworthy PA. Rochester, MN: Department of Cardiovascular Medicine, Mayo Clinic; 2019.
-
- Feigin VL, Forouzanfar MH, Krishnamurthi R, Mensah GA, Connor M, Bennett DA, Moran AE, Sacco RL, Anderson L, Truelsen T, et al.; Global Burden of Diseases, Injuries, and Risk Factors Study 2010 (GBD 2010) and the GBD Stroke Experts Group. Global and regional burden of stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet. 2014;383:245–254. doi: 10.1016/s0140-6736(13)61953-4 - DOI - PMC - PubMed
-
- Rojo-Martinez E, Sandín-Fuentes M, Calleja-Sanz AI, Cortijo-García E, García-Bermejo P, Ruiz-Piñero M, Rubio-Sanz J, Arenillas-Lara JF. High performance of an implantable Holter monitor in the detection of concealed paroxysmal atrial fibrillation in patients with cryptogenic stroke and a suspected embolic mechanism [in Spanish]. Rev Neurol. 2013;57:251–257. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
