

Pneumatosis cystoides intestinalis: a case report and literature review
- PMID: 31694581
- PMCID: PMC6836417
- DOI: 10.1186/s12876-019-1087-9
Pneumatosis cystoides intestinalis: a case report and literature review
Abstract
Background: Pneumatosis cystoides intestinalis (PCI) is a low-incidence disease that confuses many doctors. A vast number of factors are suspected to contribute to its pathogenesis, such as Crohn's disease, intestinal stenosis, ulcerative colitis, drug use, extra-gastrointestinal diseases, and chronic obstructive pulmonary disease. Most consider its pathogenesis interrelated to an increase in intra-intestinal pressure and the accumulation of gas produced by aerogenic bacteria, and patients with atypical symptoms and imaging manifestations tend to be misdiagnosed.
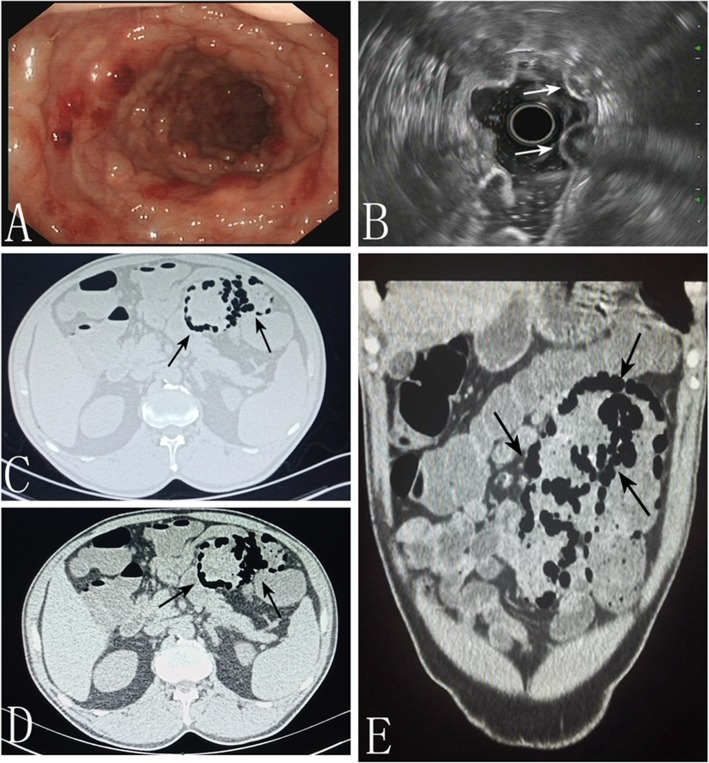
Case presentation: A 64-year-old man complained of a 3-month history of bloody stool without mucopurulent discharge, abdominal pain, or diarrhea. Colonoscopy revealed multiple nodular projections into the segmental mucosa of the sigmoid colon. Crohn's disease and malignant disease ware suspected first according to the patient's history, but laboratory examinations did not confirm either. Endoscopic ultrasound (EUS) revealed multiple cystic lesions in the submucosa. Moreover, computer tomography scan showed multiple bubble-like cysts. Combined with ultrasonography, computed tomography, and pathology findings, we ultimately made a diagnosis of PCI. Instead of surgery, we recommended conservative treatment consisting of endoscopy and oral drug administration. His symptoms improved with drug therapy after discharge, and no recurrence was noted on follow-up.
Conclusions: The incidence of PCI is low. Due to a lack of specificity in clinical manifestations and endoscopic findings, it often misdiagnosed as intestinal polyps, tumors, inflammatory bowel disease, or other conditions. Colonoscopy, computed tomography, and ultrasonography have demonstrated benefit in patients with multiple nodular projections in colon. Compared to the treatment of the above diseases, PCI treatment is effective and convenient, and the prognosis is optimistic. Therefore, clinicians should increase their awareness of PCI to avoid unnecessary misdiagnosis.
Keywords: Differential diagnosis; Pneumatosis cystoides intestinalis; Treatment.
Conflict of interest statement
The authors declare that they have no competing interests. All authors have confirmed that no support from any organization for the submitted work; no financial relationships with any organization that might have an interest in the submitted work in the previous 3 years, no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
