

Diagnostic challenge of the non-specific presentation of adult intussusception
- PMID: 31694825
- PMCID: PMC6855870
- DOI: 10.1136/bcr-2019-229931
Diagnostic challenge of the non-specific presentation of adult intussusception
Abstract
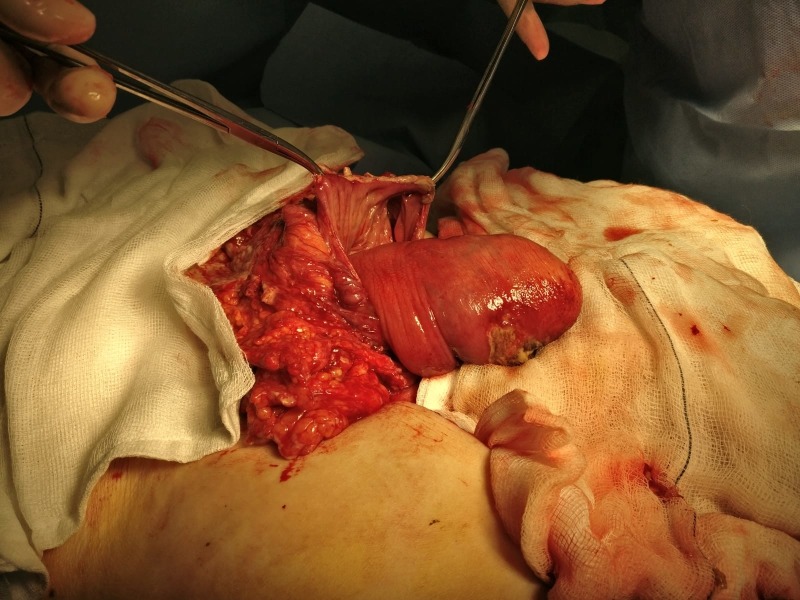
The following report will discuss the diagnosis and management of non-specific abdominal pain in a 77-year-old woman who presented to a district general hospital in South London. CT imaging demonstrated ileo-colic intussusception with free air and fluid indicating perforation. The images of the specimen clearly show the ileal tumour within the intussusception. Thus, the patient underwent an emergency right hemicolectomy and formation of a double-barrelled ileostomy. Histology subsequently confirmed this was secondary to a colonic adenocarcinoma. This case report is unique as it highlights that intussusception in adults is very difficult to accurately diagnose based on clinical features (due to non-specific findings) and even with radiology can be challenging. This is also the first documented case of the site of perforation not being directly involved with the site of intussusception. The perforation site was in fact distal to the intussusception. At the time of surgery, it was noted that the patient had significantly faecal loading up to her rectum. The resulting closed loop was the cause of her perforation.
Keywords: colon cancer; general surgery; radiology.
© BMJ Publishing Group Limited 2019. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures





Similar articles
-
Case 2. Colon cancer presenting with intestinal intussusception.J Clin Oncol. 2004 Dec 1;22(23):4853-4. doi: 10.1200/JCO.2004.02.041. J Clin Oncol. 2004. PMID: 15570090 No abstract available.
-
Intussusception revealing right colonic adenocarcinoma in a 61-year-old woman: a case report.J Med Case Rep. 2023 Jul 14;17(1):299. doi: 10.1186/s13256-023-04027-4. J Med Case Rep. 2023. PMID: 37443097 Free PMC article.
-
Transient and Non-Transient Intussusceptions of the Large Bowel in Adults: Two Case Reports.Acta Medica (Hradec Kralove). 2015;58(2):66-8. doi: 10.14712/18059694.2015.96. Acta Medica (Hradec Kralove). 2015. PMID: 26455569
-
Intermittent adult ileocecal intussusception: a case report and review of literature.Acta Clin Belg. 2014 Jan-Feb;69(1):76-81. doi: 10.1179/0001551213Z.00000000011. Acta Clin Belg. 2014. PMID: 24635405 Review.
-
Inflammatory pseudotumor of the colon causing intussusception: a case report and literature review.World J Gastroenterol. 2015 Jan 14;21(2):704-10. doi: 10.3748/wjg.v21.i2.704. World J Gastroenterol. 2015. PMID: 25593502 Free PMC article. Review.
Cited by
-
Ileocecal colonic intussusception with adenocarcinoma: A rare case report and management strategy.Int J Surg Case Rep. 2024 Mar;116:109365. doi: 10.1016/j.ijscr.2024.109365. Epub 2024 Feb 8. Int J Surg Case Rep. 2024. PMID: 38340630 Free PMC article.
References
-
- Segovia-Lohse HA. Adult intussusception with perforation and secondary peritonitis. Case report. Cir Cir 2011;79:252-55, 274-7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical