

The Prognostic and Therapeutic Role of Genomic Subtyping by Sequencing Tumor or Cell-Free DNA in Pulmonary Large-Cell Neuroendocrine Carcinoma
- PMID: 31694833
- PMCID: PMC7024651
- DOI: 10.1158/1078-0432.CCR-19-0556
The Prognostic and Therapeutic Role of Genomic Subtyping by Sequencing Tumor or Cell-Free DNA in Pulmonary Large-Cell Neuroendocrine Carcinoma
Abstract
Purpose: The optimal systemic treatment for pulmonary large-cell neuroendocrine carcinoma (LCNEC) is still under debate. Previous studies showed that LCNEC with different genomic characteristics might respond differently to different chemotherapy regimens. In this study, we sought to investigate genomic subtyping using cell-free DNA (cfDNA) analysis in advanced LCNEC and assess its potential prognostic and predictive value.
Experimental design: Tumor DNA and cfDNA from 63 patients with LCNEC were analyzed by target-captured sequencing. Survival and response analyses were applied to 54 patients with advanced stage incurable disease who received first-line chemotherapy.
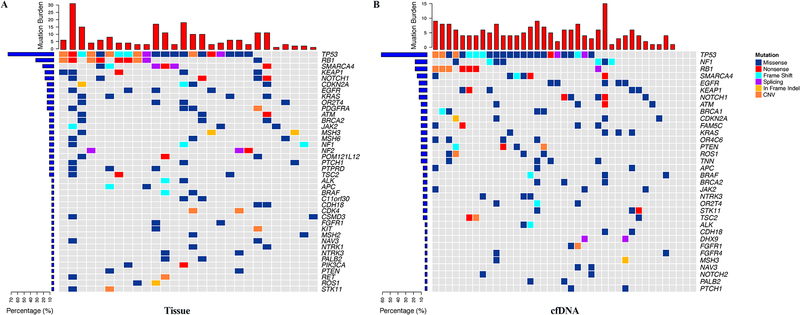
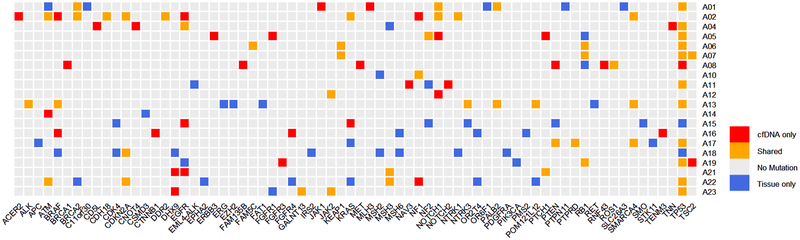
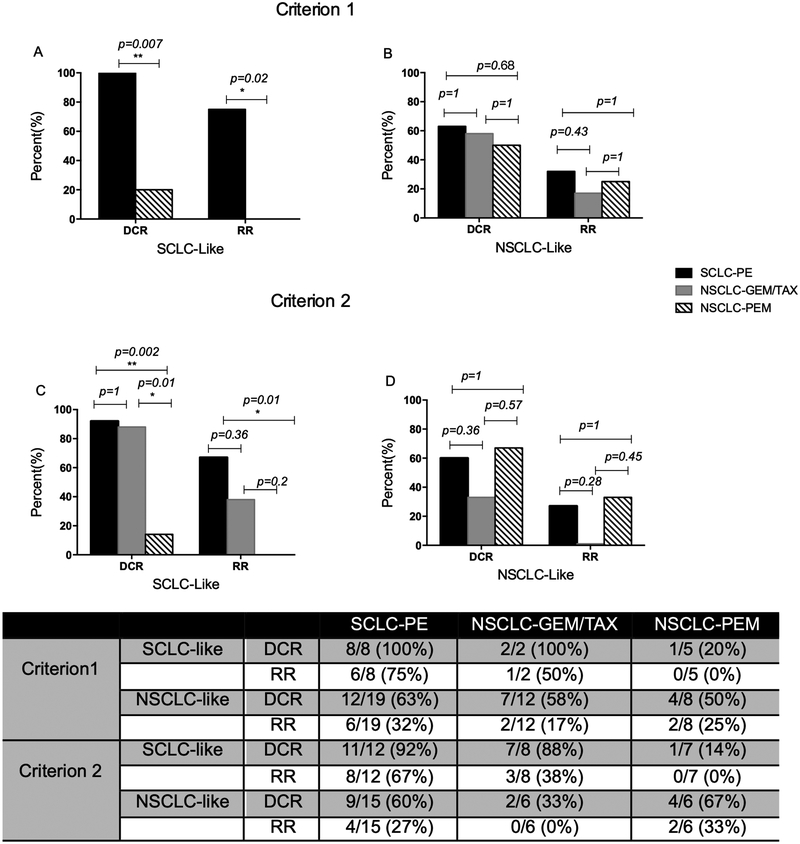
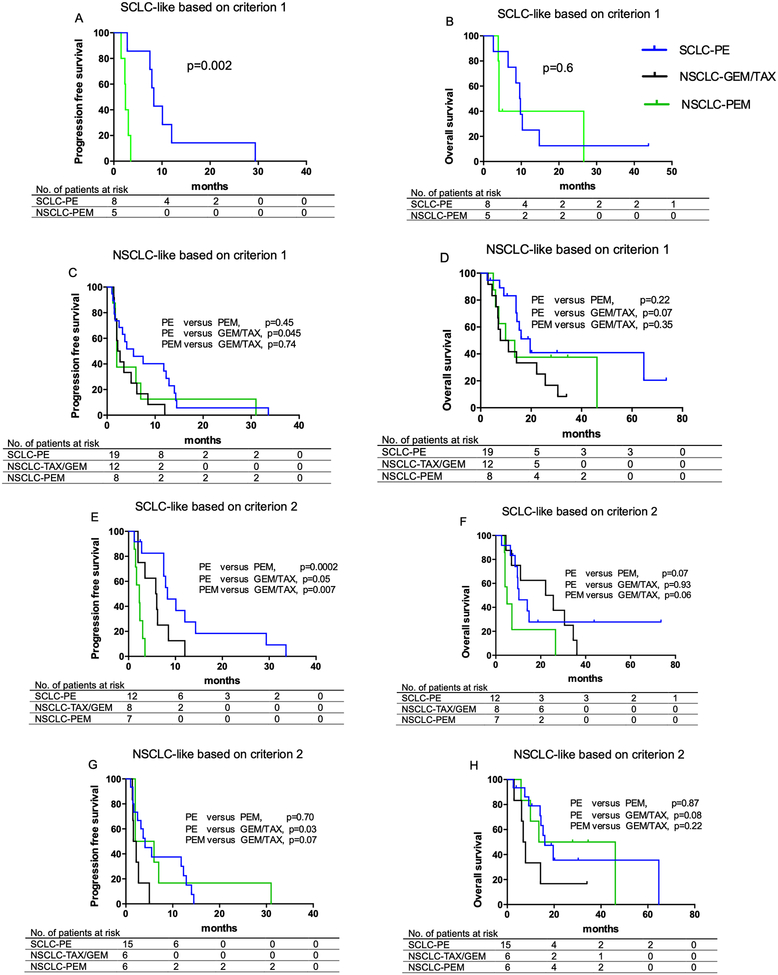
Results: The mutation landscape of frequently mutated cancer genes in LCNEC from cfDNA closely resembled that from tumor DNA, which led to a 90% concordance in genomic subtyping. The 63 patients with LCNEC were classified into small-cell lung cancer (SCLC)-like and non-small cell lung cancer (NSCLC)-like LCNEC based on corresponding genomic features derived from tumor DNA and/or cfDNA. Overall, patients with SCLC-like LCNEC had a shorter overall survival than those with NSCLC-like LCNEC despite higher response rate (RR) to chemotherapy. Furthermore, treatment with etoposide-platinum was associated with superior response and survival in SCLC-like LCNEC compared with pemetrexed-platinum and gemcitabine/taxane-platinum doublets, while treatment with gemcitabine/taxane-platinum led to a shorter survival compared with etoposide-platinum or pemetrexed-platinum in patients with NSCLC-like LCNEC.
Conclusions: Genomic subtyping has potential in prognostication and therapeutic decision-making for patients with LCNEC and cfDNA analysis may be a reliable alternative for genomic profiling of LCNEC.
©2019 American Association for Cancer Research.
Conflict of interest statement
Conflicts of interest:
Y.F.G., Y.Q.W., L.P.C., Y.H.G., L.Y., and X.Y are current employees of Geneplus-Beijing. J.V.H. is a consultant for AstraZeneca, Abbvie, Boehringer Ingelheim, Bristol-Myers Squibb, Medivation, ARIAD, Synta, Oncomed, Novartis, Genentech, and Calithera Biosciences, holds stock in Cardinal Spine LLC and Bio-Tree, and has received funding from AstraZeneca. I.I.W. receives honoraria from Roche/Genentech, Ventana, GlaxoSmithKline, Celgene, Bristol-Myers Squibb, Synta Pharmaceuticals, Boehringer Ingelheim, Medscape, Clovis, AstraZeneca, and Pfizer, and research support from Roche/Genentech, Oncoplex, and HGT. J.Z. serves as a consultant for AstraZeneca and Geneplus-Beijing and received honoraria and funding from Bristol-Myers Squibb, Merck, Roche, OrigiMed, Innovent, Bristol-Myers Squibb, Merck & Co. and Adaptive Biotechnologies Inc. outside the submitted work. The other authors declare no conflicts of interest.
Figures
Similar articles
-
Chemotherapy for pulmonary large cell neuroendocrine carcinomas: does the regimen matter?Eur Respir J. 2017 Jun 1;49(6):1601838. doi: 10.1183/13993003.01838-2016. Print 2017 Jun. Eur Respir J. 2017. PMID: 28572122 Free PMC article.
-
Large Cell Neuroendocrine Carcinoma of the Lung: Clinico-Pathologic Features, Treatment, and Outcomes.Clin Lung Cancer. 2016 Sep;17(5):e121-e129. doi: 10.1016/j.cllc.2016.01.003. Epub 2016 Jan 21. Clin Lung Cancer. 2016. PMID: 26898325 Free PMC article.
-
Role of chemotherapy and the receptor tyrosine kinases KIT, PDGFRalpha, PDGFRbeta, and Met in large-cell neuroendocrine carcinoma of the lung.J Clin Oncol. 2005 Dec 1;23(34):8774-85. doi: 10.1200/JCO.2005.02.8233. J Clin Oncol. 2005. PMID: 16314638
-
[Advances of Treatment of Pulmonary Large Cell Neuroendocrine Carcinoma].Zhongguo Fei Ai Za Zhi. 2024 Aug 20;27(8):622-628. doi: 10.3779/j.issn.1009-3419.2024.102.28. Zhongguo Fei Ai Za Zhi. 2024. PMID: 39318255 Free PMC article. Review. Chinese.
-
Different Characteristics and Survival between Surgically Resected Pure and Combined Pulmonary Large Cell Neuroendocrine Carcinoma.Ann Surg Oncol. 2022 Sep;29(9):5666-5678. doi: 10.1245/s10434-022-11610-4. Epub 2022 May 11. Ann Surg Oncol. 2022. PMID: 35543906 Review.
Cited by
-
Two case reports: EML4-ALK rearrangement large cell neuroendocrine carcinoma and literature review.Front Oncol. 2023 Nov 1;13:1227980. doi: 10.3389/fonc.2023.1227980. eCollection 2023. Front Oncol. 2023. PMID: 38023218 Free PMC article.
-
Comprehensive Genomic Profiling of Rare Tumors: Routes to Targeted Therapies.Front Oncol. 2020 Apr 21;10:536. doi: 10.3389/fonc.2020.00536. eCollection 2020. Front Oncol. 2020. PMID: 32373528 Free PMC article.
-
Molecular features of gastroenteropancreatic neuroendocrine carcinoma: A comparative analysis with lung neuroendocrine carcinoma and digestive adenocarcinomas.Chin J Cancer Res. 2024 Feb 29;36(1):90-102. doi: 10.21147/j.issn.1000-9604.2024.01.09. Chin J Cancer Res. 2024. PMID: 38455367 Free PMC article.
-
Long-term survival in advanced pulmonary large-cell neuroendocrine carcinoma after multi-line immunochemotherapy and anti-angiogenic therapy: a case report.Front Immunol. 2025 Jun 30;16:1618672. doi: 10.3389/fimmu.2025.1618672. eCollection 2025. Front Immunol. 2025. PMID: 40661961 Free PMC article.
-
Risk factors, survival analysis, and nomograms for distant metastasis in patients with primary pulmonary large cell neuroendocrine carcinoma: A population-based study.Front Endocrinol (Lausanne). 2022 Oct 17;13:973091. doi: 10.3389/fendo.2022.973091. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36329892 Free PMC article.
References
-
- Travis WD, Linnoila RI, Tsokos MG, Hitchcock CL, Cutler GB Jr., Nieman L, et al. Neuroendocrine tumors of the lung with proposed criteria for large-cell neuroendocrine carcinoma. An ultrastructural, immunohistochemical, and flow cytometric study of 35 cases. Am J Surg Pathol 1991;15(6):529–53. - PubMed
-
- Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG. Introduction to The 2015 World Health Organization Classification of Tumors of the Lung, Pleura, Thymus, and Heart. Journal of thoracic oncology : official publication of the International Association for the Study of Lung Cancer 2015;10(9):1240–2 doi 10.1097/JTO.0000000000000663. - DOI - PubMed
-
- Jones MH, Virtanen C, Honjoh D, Miyoshi T, Satoh Y, Okumura S, et al. Two prognostically significant subtypes of high-grade lung neuroendocrine tumours independent of small-cell and large-cell neuroendocrine carcinomas identified by gene expression profiles. Lancet 2004;363(9411):775–81 doi 10.1016/S0140-6736(04)15693-6. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
