

Complement Activation and Thrombotic Microangiopathies
- PMID: 31694864
- PMCID: PMC6895490
- DOI: 10.2215/CJN.05830519
Complement Activation and Thrombotic Microangiopathies
Abstract
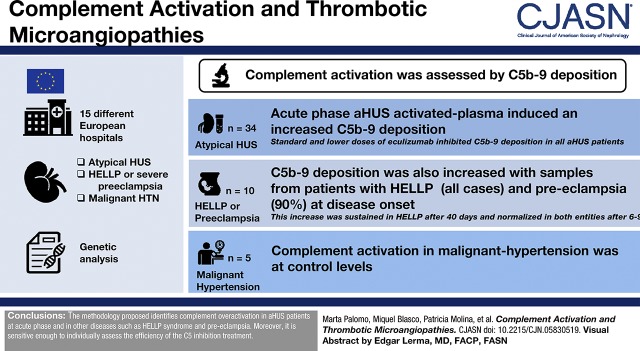
Background and objectives: Atypical hemolytic uremic syndrome is a form of thrombotic microangiopathy caused by dysregulation of the alternative complement pathway. There is evidence showing complement activation in other thrombotic microangiopathies. The aim of this study was to evaluate complement activation in different thrombotic microangiopathies and to monitor treatment response.
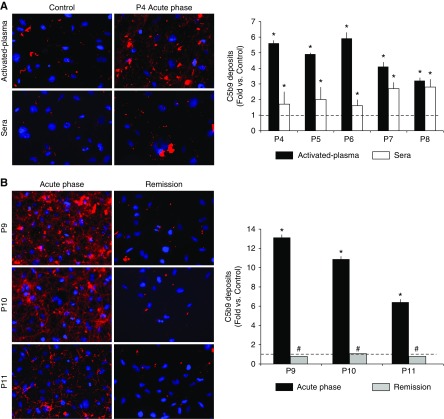
Design, setting, participants, & measurements: Complement activation was assessed by exposing endothelial cells to sera or activated-patient plasma-citrated plasma mixed with a control sera pool (1:1)-to analyze C5b-9 deposits by immunofluorescence. Patients with atypical hemolytic uremic syndrome (n=34) at different stages of the disease, HELLP syndrome (a pregnancy complication characterized by hemolysis, elevated liver enzymes, and low platelet count) or severe preeclampsia (n=10), and malignant hypertension (n=5) were included.
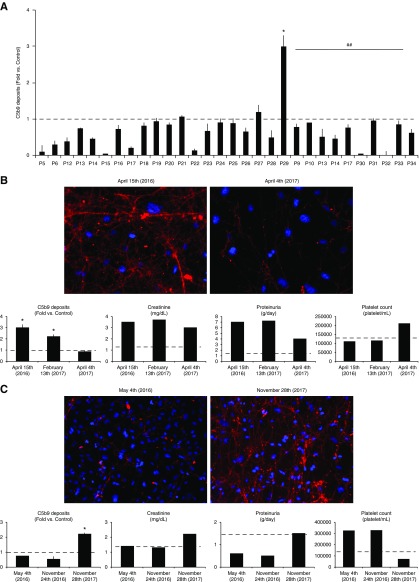
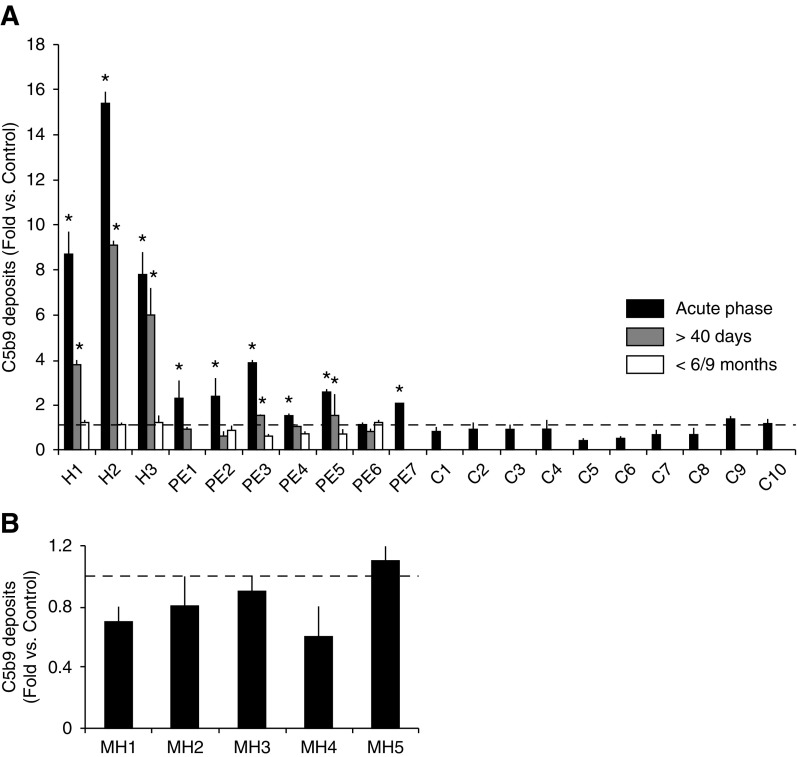
Results: Acute phase atypical hemolytic uremic syndrome-activated plasma induced an increased C5b-9 deposition on endothelial cells. Standard and lower doses of eculizumab inhibited C5b-9 deposition in all patients with atypical hemolytic uremic syndrome, except in two who showed partial remission and clinical relapse. Significant fibrin formation was observed together with C5b-9 deposition. Results obtained using activated-plasma samples were more marked and reproducible than those obtained with sera. C5b-9 deposition was also increased with samples from patients with HELLP (all cases) and preeclampsia (90%) at disease onset. This increase was sustained in those with HELLP after 40 days, and levels normalized in patients with both HELLP and preeclampsia after 6-9 months. Complement activation in those with malignant hypertension was at control levels.
Conclusions: The proposed methodology identifies complement overactivation in patients with atypical hemolytic uremic syndrome at acute phase and in other diseases such as HELLP syndrome and preeclampsia. Moreover, it is sensitive enough to individually assess the efficiency of the C5 inhibition treatment.
Keywords: HELLP syndrome; alternative; antibodies; atypical hemolytic uremic syndrome; complement C9; complement activation; complement membrane; complement pathway; complement system proteins; eculizumab; endothelial cells; female; fibrin; fluorescent antibody technique; humanized; humans; hypertension; malignant; monoclonal; pre-eclampsia; pregnancy; recurrence; thrombotic microangiopathies.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
-
Monitoring Complement Activation: The New Conundrum in Thrombotic Microangiopathies.Clin J Am Soc Nephrol. 2019 Dec 6;14(12):1682-1683. doi: 10.2215/CJN.12111019. Epub 2019 Nov 6. Clin J Am Soc Nephrol. 2019. PMID: 31811084 Free PMC article. No abstract available.
References
-
- George JN, Nester CM: Syndromes of thrombotic microangiopathy. N Engl J Med 371: 654–666, 2014 - PubMed
-
- Sethi S, Fervenza FC: Pathology of renal diseases associated with dysfunction of the alternative pathway of complement: C3 glomerulopathy and atypical hemolytic uremic syndrome (aHUS). Semin Thromb Hemost 40: 416–421, 2014 - PubMed
-
- Román E, Mendizábal S, Jarque I, de la Rubia J, Sempere A, Morales E, Praga M, Ávila A, Górriz JL: Secondary thrombotic microangiopathy and eculizumab: A reasonable therapeutic option. Nefrologia 37: 478–491, 2017 - PubMed
-
- Cavero T, Rabasco C, López A, Román E, Ávila A, Sevillano Á, Huerta A, Rojas-Rivera J, Fuentes C, Blasco M, Jarque A, García A, Mendizabal S, Gavela E, Macía M, Quintana LF, María Romera A, Borrego J, Arjona E, Espinosa M, Portolés J, Gracia-Iguacel C, González-Parra E, Aljama P, Morales E, Cao M, Rodríguez de Córdoba S, Praga M: Eculizumab in secondary atypical haemolytic uraemic syndrome. Nephrol Dial Transplant 32: 466–474, 2017 - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
