

Weight Loss and Illness Severity in Adolescents With Atypical Anorexia Nervosa
- PMID: 31694978
- PMCID: PMC6889949
- DOI: 10.1542/peds.2019-2339
Weight Loss and Illness Severity in Adolescents With Atypical Anorexia Nervosa
Abstract
Background: Lower weight has historically been equated with more severe illness in anorexia nervosa (AN). Reliance on admission weight to guide clinical concern is challenged by the rise in patients with atypical anorexia nervosa (AAN) requiring hospitalization at normal weight.
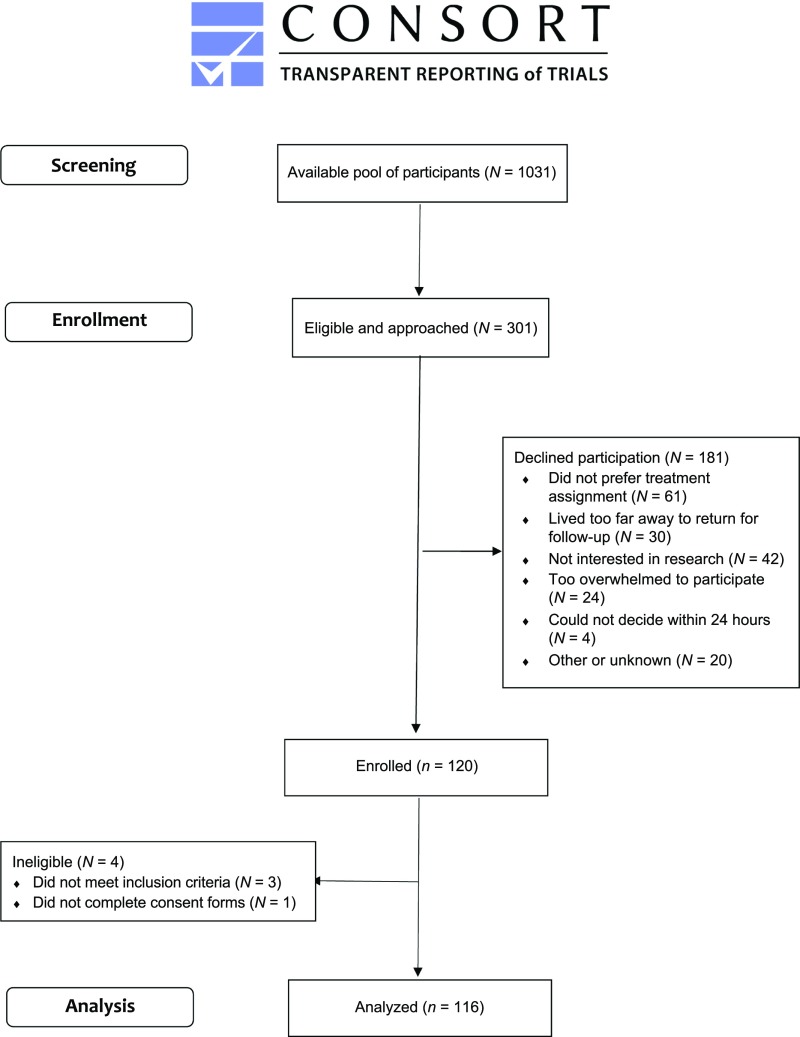
Methods: We examined weight history and illness severity in 12- to 24-year-olds with AN (n = 66) and AAN (n = 50) in a randomized clinical trial, the Study of Refeeding to Optimize Inpatient Gains (www.clinicaltrials.gov; NCT02488109). Amount of weight loss was the difference between the highest historical percentage median BMI and admission; rate was the amount divided by duration (months). Unpaired t tests compared AAN and AN; multiple variable regressions examined associations between weight history variables and markers of illness severity at admission. Stepwise regression examined the explanatory value of weight and menstrual history on selected markers.
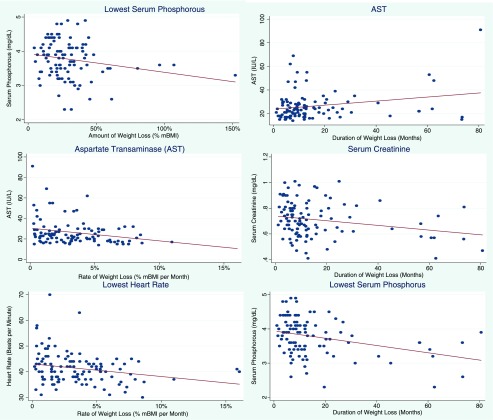
Results: Participants were 16.5 ± 2.6 years old, and 91% were of female sex. Groups did not differ by weight history or admission heart rate (HR). Eating Disorder Examination Questionnaire global scores were higher in AAN (mean 3.80 [SD 1.66] vs mean 3.00 [SD 1.66]; P = .02). Independent of admission weight, lower HR (β = -0.492 [confidence interval (CI) -0.883 to -0.100]; P = .01) was associated with faster loss; lower serum phosphorus was associated with a greater amount (β = -0.005 [CI -0.010 to 0.000]; P = .04) and longer duration (β = -0.011 [CI -0.017 to 0.005]; P = .001). Weight and menstrual history explained 28% of the variance in HR and 36% of the variance in serum phosphorus.
Conclusions: Weight history was independently associated with markers of malnutrition in inpatients with restrictive eating disorders across a range of body weights and should be considered when assessing illness severity on hospital admission.
Copyright © 2019 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
References
-
- Miller KK, Grinspoon SK, Ciampa J, et al. . Medical findings in outpatients with anorexia nervosa. Arch Intern Med. 2005;165(5):561–566 - PubMed
-
- Misra M, Aggarwal A, Miller KK, et al. . Effects of anorexia nervosa on clinical, hematologic, biochemical, and bone density parameters in community-dwelling adolescent girls. Pediatrics. 2004;114(6):1574–1583 - PubMed
-
- Ornstein RM, Golden NH, Jacobson MS, Shenker IR. Hypophosphatemia during nutritional rehabilitation in anorexia nervosa: implications for refeeding and monitoring. J Adolesc Health. 2003;32(1):83–88 - PubMed
