

Prevalence Of Chronic Hypercapnia In Severe Chronic Obstructive Pulmonary Disease: Data From The HOmeVent Registry
- PMID: 31695357
- PMCID: PMC6805244
- DOI: 10.2147/COPD.S222803
Prevalence Of Chronic Hypercapnia In Severe Chronic Obstructive Pulmonary Disease: Data From The HOmeVent Registry
Abstract
Background: Non-invasive ventilation (NIV) has been shown to improve survival and quality of life in COPD patients with chronic hypercapnic respiratory failure. However, the proportion of COPD patients with chronic hypercapnia is not yet known and clinical data enabling better identification of patients are scarce. The HOmeVent registry was initiated to determine the prevalence of chronic hypercapnia in COPD in an outpatient setting and to evaluate the predictors of hypercapnia.
Methods: HOmeVent is a multicenter, prospective, observational, non-interventional patient registry that includes COPD patients in GOLD stage 3 or 4. Eligible patients were identified and enrolled in an outpatient setting during routine clinic visits. Assessments included blood gas analyses, pulmonary function testing and quality of life assessment.
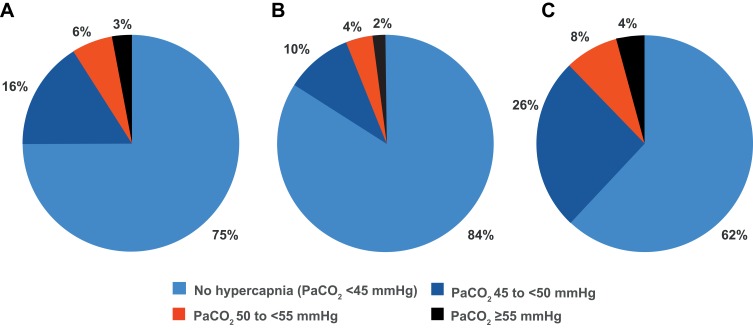
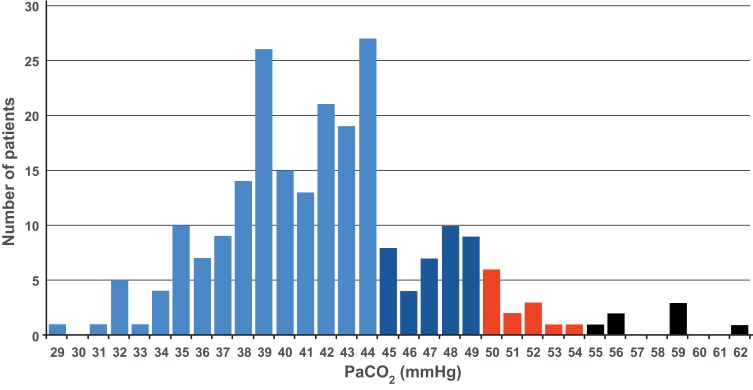
Results: Ten outpatient clinics in Germany enrolled 231 COPD patients in the registry (135 in GOLD stage 3 (58%) and 96 in GOLD stage 4 (42%)). Arterial carbon dioxide pressure (PaCO2) was ≥45 mmHg in 58 patients (25%); of these, 20 (9%) had PaCO2 ≥50 mmHg. The prevalence of hypercapnia at both cut-off values was numerically higher for patients in GOLD stage 4 versus 3. An increased body mass index, a decreased forced vital capacity and an increased bicarbonate level were significant independent predictors of hypercapnia. The proportion of patients who received NIV was 6% overall and 22% of those with hypercapnia.
Conclusion: A relevant proportion of COPD patients in GOLD stage 3 and 4 exhibits chronic hypercapnia and might, therefore, be candidates for long-term domiciliary NIV treatment.
Keywords: chronic obstructive pulmonary disease; hypercapnia; non-invasive ventilation; quality of life; registry.
© 2019 Dreher et al.
Conflict of interest statement
MD has received speaking and advisor fees from Phillips, Weinmann, and Heinen und Löwenstein, during the conduct of the study. WW has received speaking fees and advisory fees from Weinmann, Vivisol, Heinen und Löwenstein, VitalAire (all in Germany) and from Philips-REspironics (USA) ; in addition, the Cologne study group has received open research grants from Weinmann, Vivisol, Heinen und Löwenstein and VitalAire (all in Germany), and from Philips-Respironics (USA). HW is a paid consultant to ResMed. TF is Chief Executive Officer at the Clinical Research Institute which was in charge of the HOmeVent registry. PCN, DM and A Graml are employees of ResMed. A Gröschel reports personal fees from ResMed, during the conduct of the study. TK and GH have no conflicts of interest to disclose beyond financial support for the HOmeVent registry. The authors report no other conflicts of interest in this work.
Figures
References
-
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(9):691–706. doi:10.1016/S2213-2600(17)30293-X - DOI - PMC - PubMed
-
- Foreman KJ, Marquez N, Dolgert A, et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet. 2018;392(10159):2052–2090. doi:10.1016/S0140-6736(18)31694-5 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
