

Cytomegalovirus infection is a risk factor for tuberculosis disease in infants
- PMID: 31697647
- PMCID: PMC6962026
- DOI: 10.1172/jci.insight.130090
Cytomegalovirus infection is a risk factor for tuberculosis disease in infants
Abstract
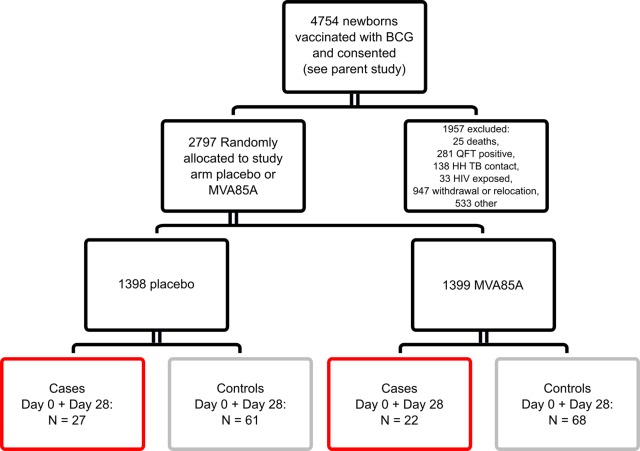
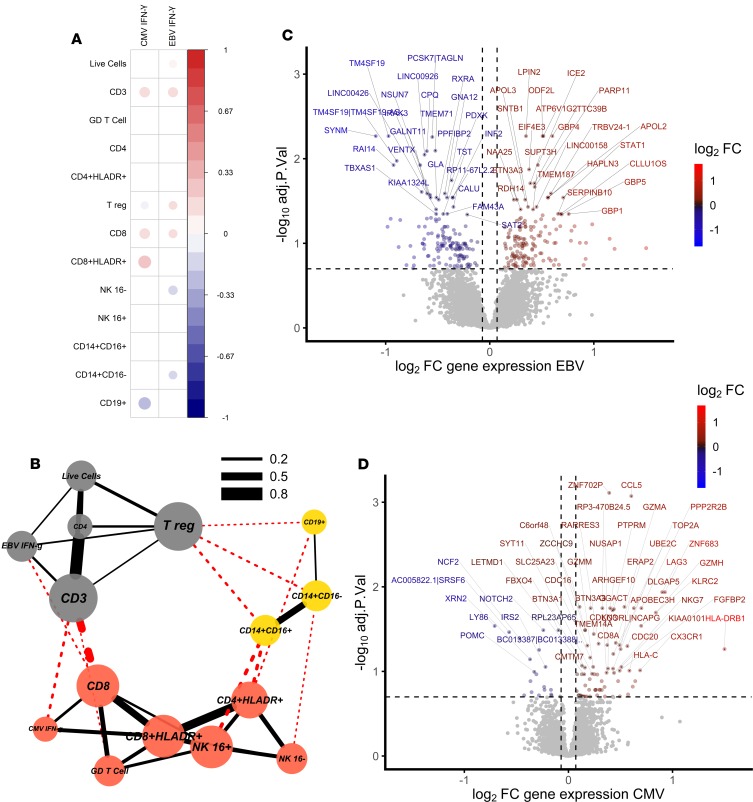
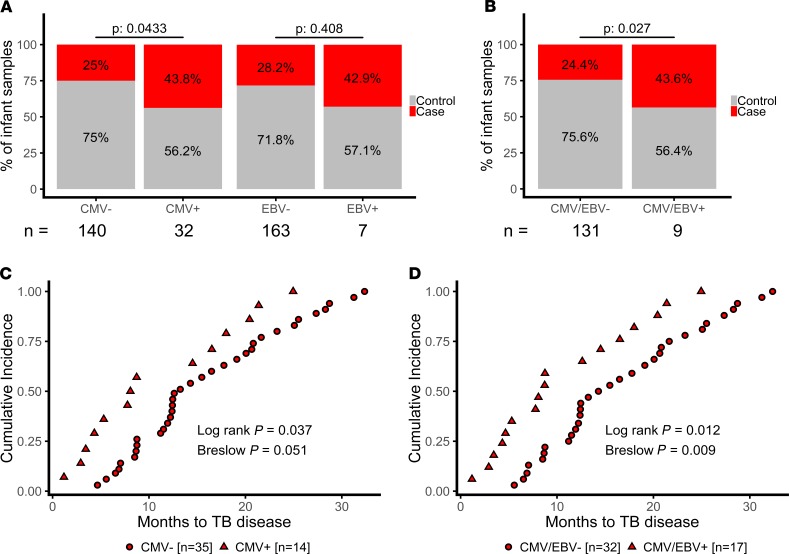
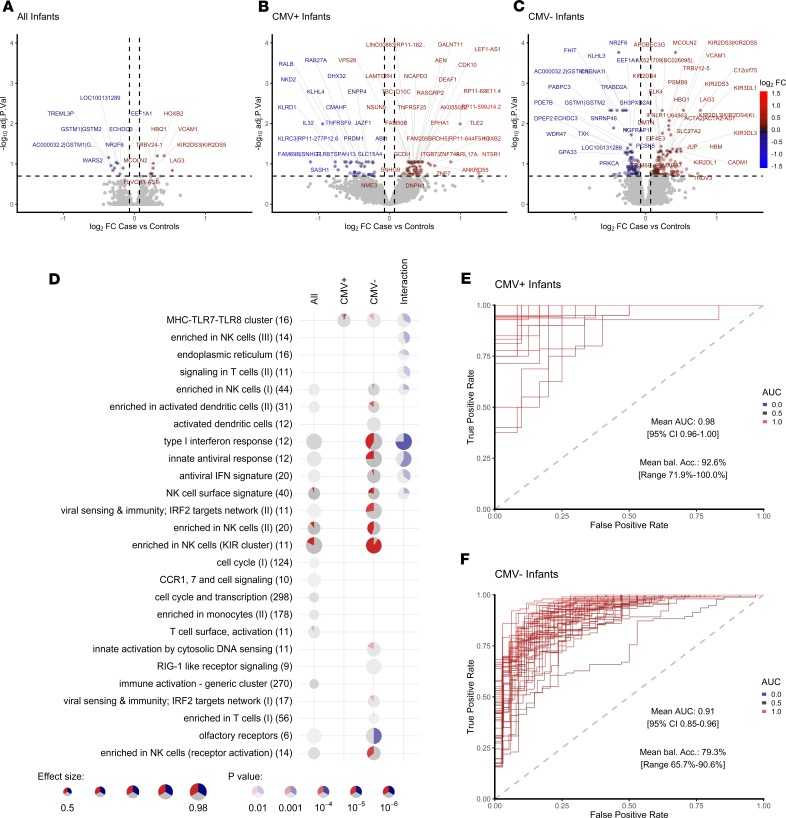
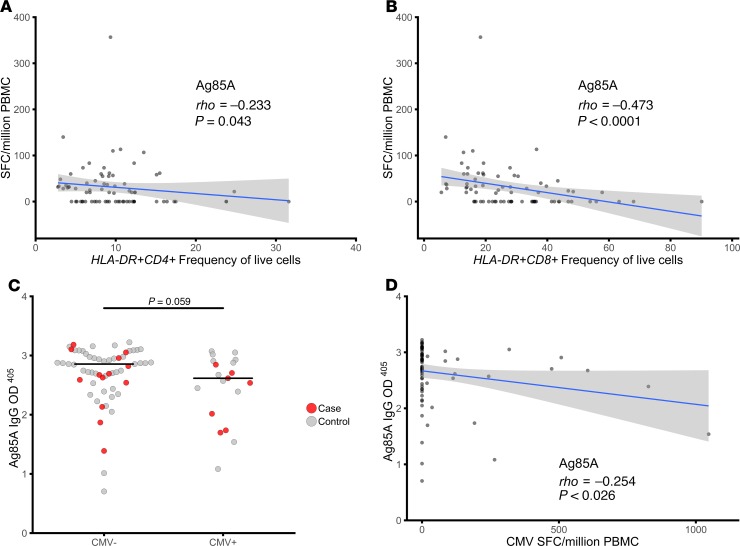
Immune activation is associated with increased risk of tuberculosis (TB) disease in infants. We performed a case-control analysis to identify drivers of immune activation and disease risk. Among 49 infants who developed TB disease over the first 2 years of life, and 129 healthy matched controls, we found the cytomegalovirus-stimulated (CMV-stimulated) IFN-γ response to be associated with CD8+ T cell activation (Spearman's rho, P = 6 × 10-8). A CMV-specific IFN-γ response was also associated with increased risk of developing TB disease (conditional logistic regression; P = 0.043; OR, 2.2; 95% CI, 1.02-4.83) and shorter time to TB diagnosis (Log Rank Mantel-Cox, P = 0.037). CMV+ infants who developed TB disease had lower expression of NK cell-associated gene signatures and a lower frequency of CD3-CD4-CD8- lymphocytes. We identified transcriptional signatures predictive of TB disease risk among CMV ELISpot-positive (area under the receiver operating characteristic [AUROC], 0.98, accuracy, 92.57%) and -negative (AUROC, 0.9; accuracy, 79.3%) infants; the CMV- signature was validated in an independent infant study (AUROC, 0.71; accuracy, 63.9%). A 16-gene signature that previously identified adolescents at risk of developing TB disease did not accurately classify case and control infants in this study. Understanding the microbial drivers of T cell activation, such as CMV, could guide new strategies for prevention of TB disease in infants.
Trial registration: ClinicalTrials.gov NCT00953927.
Keywords: Inflammation; NK cells; Tuberculosis; Vaccines.
Conflict of interest statement
Figures
References
-
- [No authors listed]. World Health Organization Global Tuberculosis Report 2019. World Health Organization. https://www.who.int/tb/publications/global_report/en/ Accessed October 31, 2019.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
