

Effects of virtual reality rehabilitation training on gait and balance in patients with Parkinson's disease: A systematic review
- PMID: 31697777
- PMCID: PMC6837756
- DOI: 10.1371/journal.pone.0224819
Effects of virtual reality rehabilitation training on gait and balance in patients with Parkinson's disease: A systematic review
Abstract
Objective: In recent years, virtual reality (VR) has been tested as a therapeutic tool in neurorehabilitation research. However, the impact effectiveness of VR technology on for Parkinson's Disease (PD) patients is still remains controversial unclear. In order to provide a more scientific basis for rehabilitation of PD patients' modality, we conducted a systematic review of VR rehabilitation training for PD patients and focused on the improvement of gait and balance.
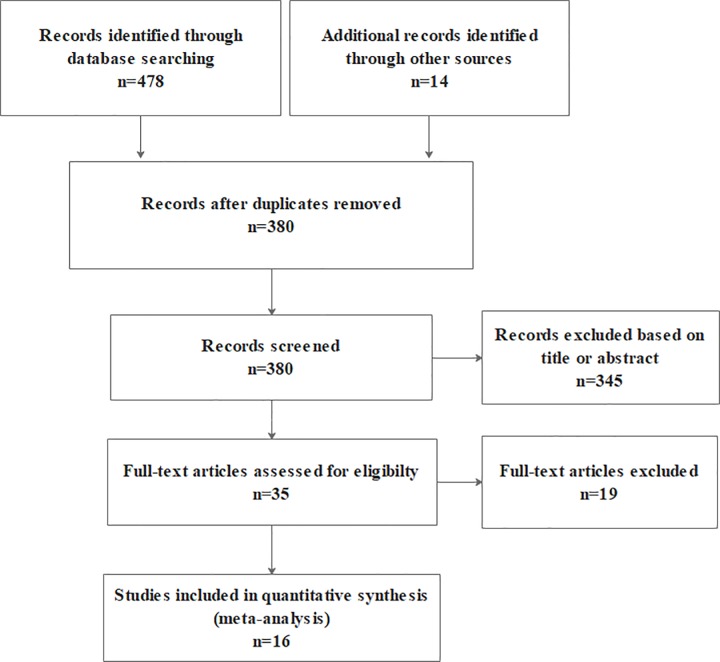
Methods: An comprehensive search was conducted using the following databases: PubMed, Web of Science, Cochrane Library, CINHAL, Embase and CNKI (China National Knowledge Infrastructure).Articles published before 30 December 2018 and of a randomized controlled trial design to study the effects of VR for patients with PD were included. The study data were pooled and a meta-analysis was completed. This systematic review was conducted in accordance with the PRISMA guideline statement and was registered in the PROSPERO database (CRD42018110264).
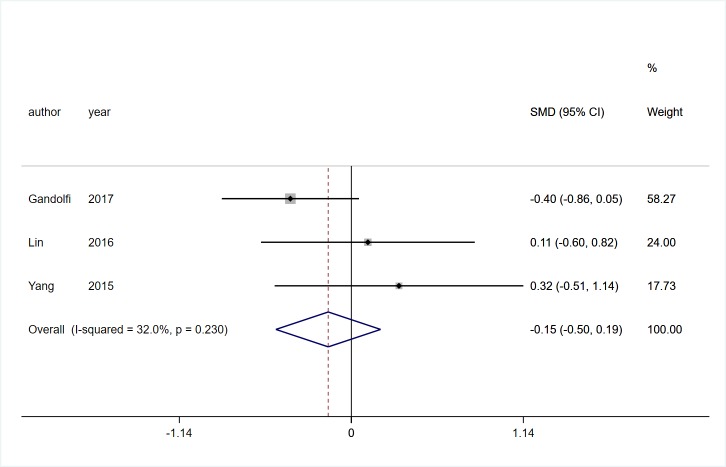
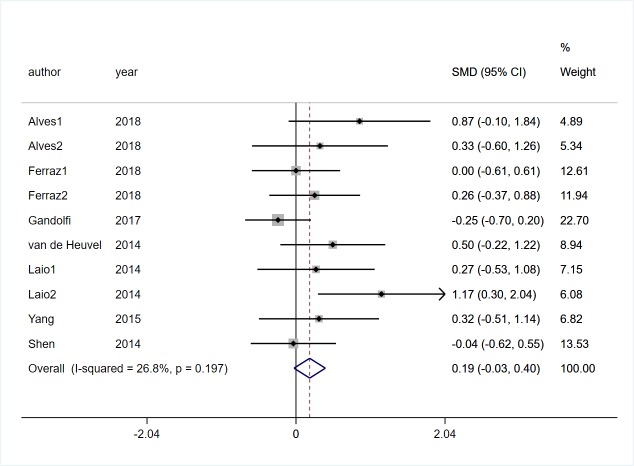
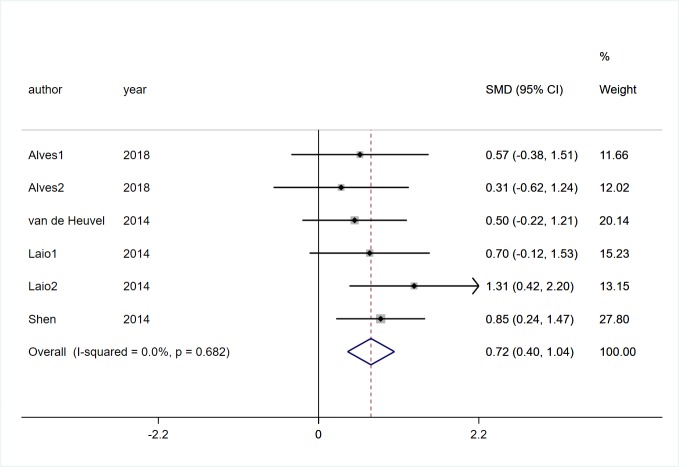
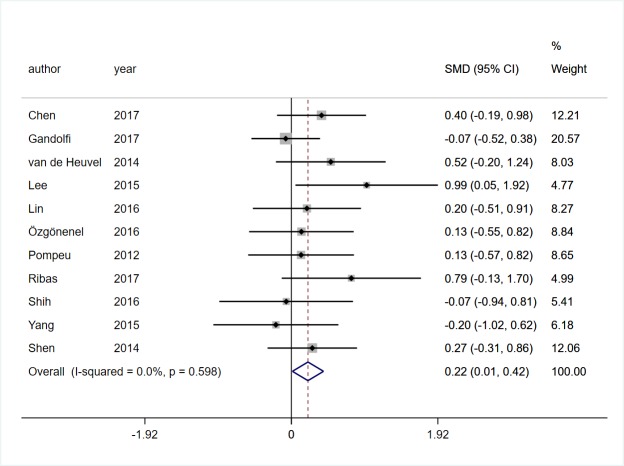
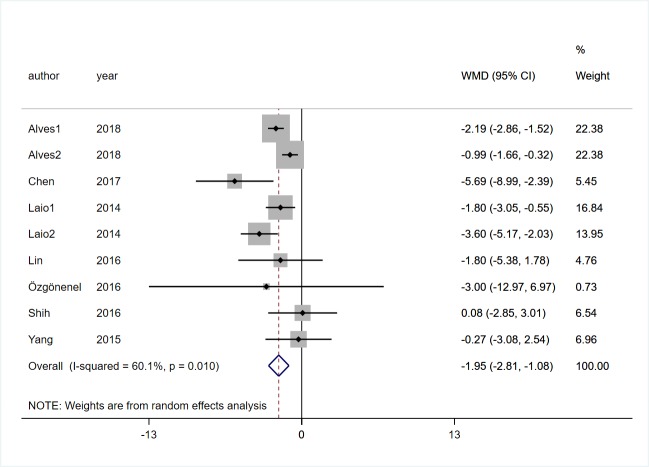
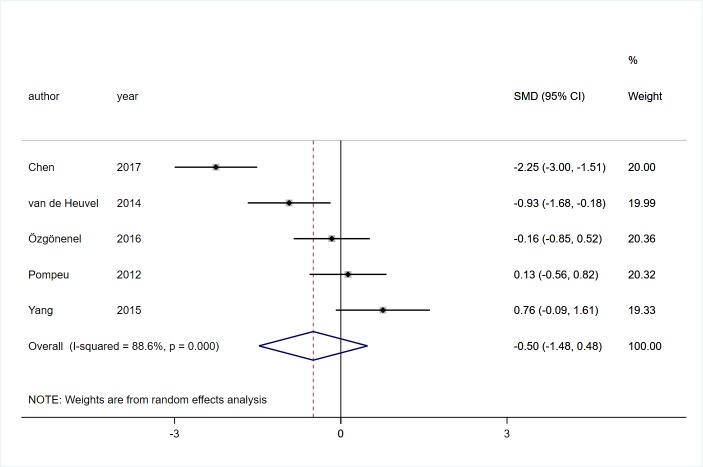
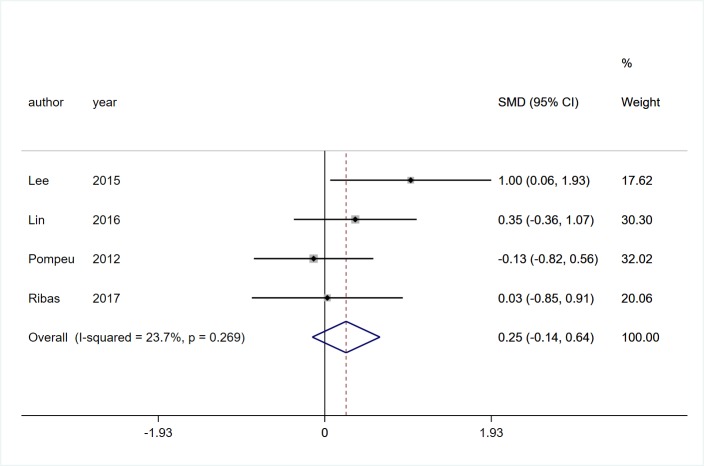
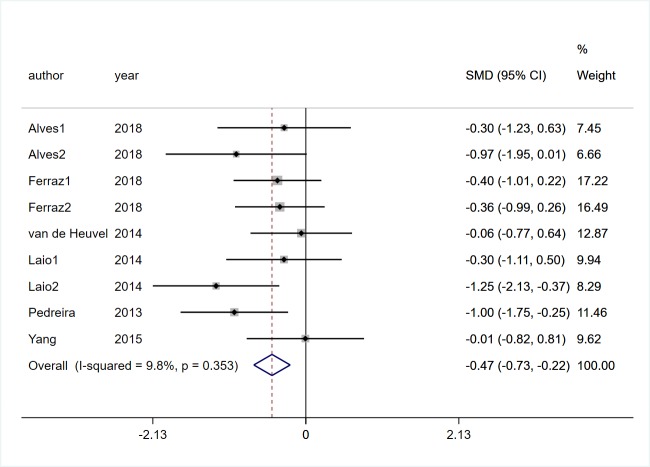
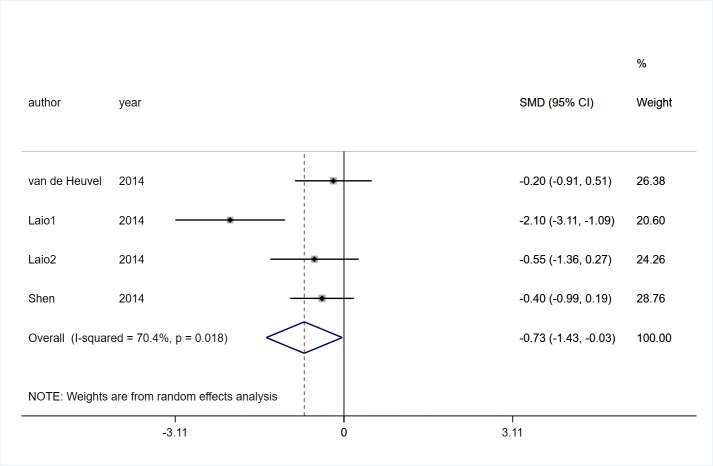
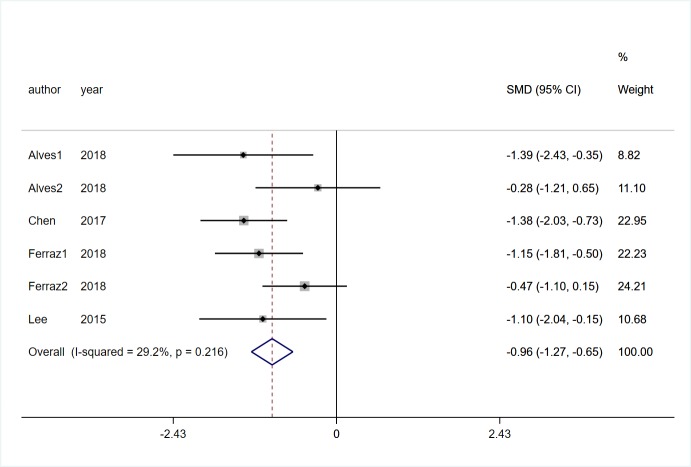
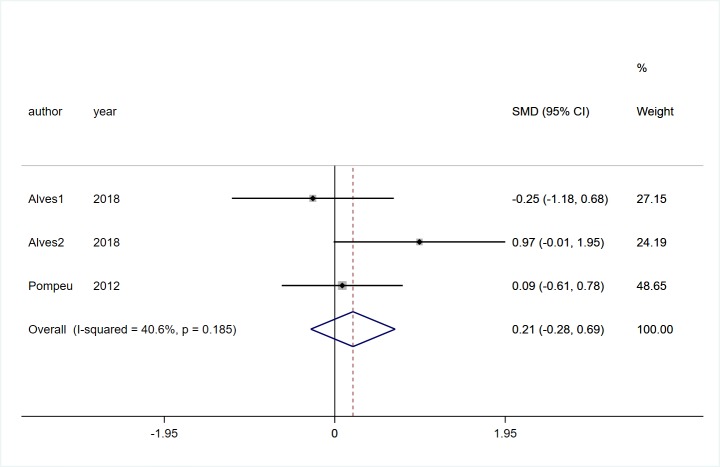
Results: A total of sixteen articles involving 555 participants with PD were included in our analysis. VR rehabilitation training performed better than conventional or traditional rehabilitation training in three aspects: step and stride length (SMD = 0.72, 95%CI = 0.40,1.04, Z = 4.38, P<0.01), balance function (SMD = 0.22, 95%CI = 0.01,0.42, Z = 2.09, P = 0.037), and mobility(MD = -1.95, 95%CI = -2.81,-1.08, Z = 4.41, P<0.01). There was no effect on the dynamic gait index (SMD = -0.15, 95%CI = -0.50,0.19, Z = 0.86, P = 0.387), and gait speed (SMD = 0.19, 95%CI = -0.03,0.40, Z = 1.71, P = 0.088).As for the secondary outcomes, compared with the control group, VR rehabilitation training demonstrated more significant effects on the improvement of quality of life (SMD = -0.47, 95%CI = -0.73,-0.22, Z = 3.64, P<0.01), level of confidence (SMD = -0.73, 95%CI = -1.43,-0.03, Z = 2.05, P = 0.040), and neuropsychiatric symptoms (SMD = -0.96, 95%CI = -1.27,-0.65, Z = 6.07, P<0.01), while it may have similar effects on global motor function (SMD = -0.50, 95%CI = -1.48,0.48, Z = 0.99, P = 0.32), activities of daily living (SMD = 0.25, 95%CI = -0.14,0.64, Z = 1.24, P = 0.216), and cognitive function (SMD = 0.21, 95%CI = -0.28,0.69, Z = 0.84, P = 0.399).During the included interventions, four patients developed mild dizziness and one patient developed severe dizziness and vomiting.
Conclusions: According to the results of this study, we found that VR rehabilitation training can not only achieve the same effect as conventional rehabilitation training. Moreover, it has better performance on gait and balance in patients with PD. Taken together, when the effect of traditional rehabilitation training on gait and balance of PD patients is not good enough, we believe that VR rehabilitation training can at least be used as an alternative therapy. More rigorous design of large-sample, multicenter randomized controlled trials are needed to provide a stronger evidence-based basis for verifying its potential advantages.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
The role of virtual reality on outcomes in rehabilitation of Parkinson's disease: meta-analysis and systematic review in 1031 participants.Neurol Sci. 2020 Mar;41(3):529-536. doi: 10.1007/s10072-019-04144-3. Epub 2019 Dec 6. Neurol Sci. 2020. PMID: 31808000 Free PMC article.
-
Efficacy of Virtual Reality-Based Interventions on Cognitive Function in Patients With Neuropsychiatric Disorders: Systematic Review and Meta-Analysis of Randomized Controlled Trials.JMIR Serious Games. 2025 May 8;13:e67501. doi: 10.2196/67501. JMIR Serious Games. 2025. PMID: 40341171 Free PMC article. Review.
-
Effects of immersive and non-immersive virtual reality-based rehabilitation training on cognition, motor function, and daily functioning in patients with mild cognitive impairment or dementia: A systematic review and meta-analysis.Clin Rehabil. 2024 Mar;38(3):305-321. doi: 10.1177/02692155231213476. Epub 2023 Nov 20. Clin Rehabil. 2024. PMID: 38289618
-
Efficacy of virtual reality training on motor performance, activity of daily living, and quality of life in patients with Parkinson's disease: an umbrella review comprising meta-analyses of randomized controlled trials.J Neuroeng Rehabil. 2023 Sep 30;20(1):133. doi: 10.1186/s12984-023-01256-y. J Neuroeng Rehabil. 2023. PMID: 37777748 Free PMC article.
-
Effect of virtual reality rehabilitation on functional outcomes for return-to-work patients with Parkinson's disease: An umbrella review of systematic reviews.NeuroRehabilitation. 2022;51(2):201-211. doi: 10.3233/NRE-220029. NeuroRehabilitation. 2022. PMID: 35599505
Cited by
-
Comparing balance using the BESTest in Alzheimer, Huntington and Parkinson disease.Neurodegener Dis Manag. 2024;14(3-4):87-96. doi: 10.1080/17582024.2024.2388507. Epub 2024 Aug 19. Neurodegener Dis Manag. 2024. PMID: 39155806 Free PMC article.
-
Developing an Immersive Virtual Reality Training System for Novel Pediatric Power Wheelchair Users: Protocol for a Feasibility Study.JMIR Res Protoc. 2022 Oct 6;11(10):e39140. doi: 10.2196/39140. JMIR Res Protoc. 2022. PMID: 36201405 Free PMC article.
-
Using virtual reality to prepare patients for radiotherapy: A systematic review of interventional studies with educational sessions.Tech Innov Patient Support Radiat Oncol. 2023 Feb 24;25:100203. doi: 10.1016/j.tipsro.2023.100203. eCollection 2023 Mar. Tech Innov Patient Support Radiat Oncol. 2023. PMID: 36873800 Free PMC article. Review.
-
Wearable rehabilitation wristband for distal radius fractures.Front Neurosci. 2023 Sep 14;17:1238176. doi: 10.3389/fnins.2023.1238176. eCollection 2023. Front Neurosci. 2023. PMID: 37781255 Free PMC article.
-
The Challenges and Perspectives of the Integration Between Virtual and Augmented Reality and Manual Therapies.Front Neurol. 2021 Jun 30;12:700211. doi: 10.3389/fneur.2021.700211. eCollection 2021. Front Neurol. 2021. PMID: 34276550 Free PMC article. Review.
References
-
- Canning CG, Paul SS, Alice N. Prevention of falls in Parkinson's disease: a review of fall risk factors and the role of physical interventions. Neurodegener Dis Manag. 2014; 3: 203–221. - PubMed
-
- Jankovic J. Parkinson's disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry. 2008; 4: 368–376. - PubMed
-
- Rizos A, Martinezmartin P, Odin P, Antonini A, Kessel B, Kozul TK,et al. Characterizing motor and non-motor aspects of early-morning off periods in Parkinson's disease: An international multicenter study. Parkinsonism Relat Disord. 2014; 11: 1231–1235. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
