

A multicenter, open-label phase 3 study of emicizumab prophylaxis in children with hemophilia A with inhibitors
- PMID: 31697801
- PMCID: PMC6908828
- DOI: 10.1182/blood.2019001869
A multicenter, open-label phase 3 study of emicizumab prophylaxis in children with hemophilia A with inhibitors
Abstract
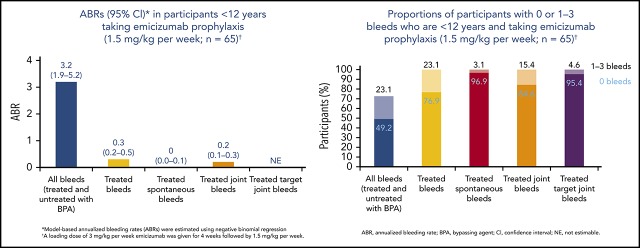
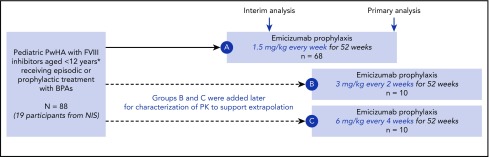
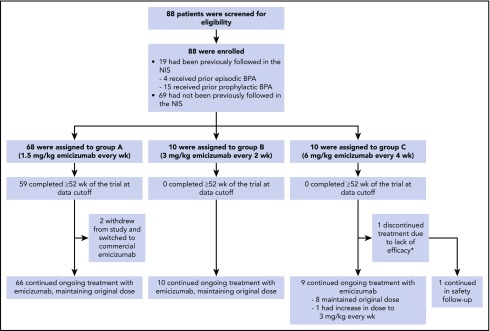
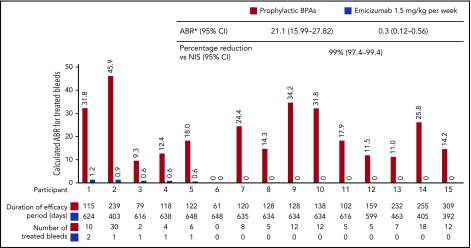
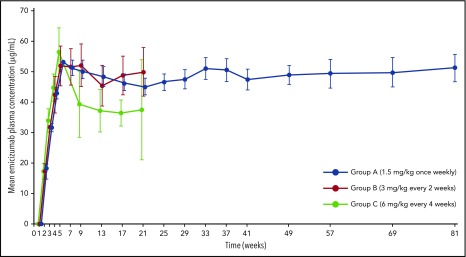
Emicizumab, a bispecific humanized monoclonal antibody, bridges activated factor IX (FIX) and FX to restore the function of missing activated FVIII in hemophilia A. Emicizumab prophylaxis in children with hemophilia A and FVIII inhibitors was investigated in a phase 3 trial (HAVEN 2). Participants, previously receiving episodic/prophylactic bypassing agents (BPAs), were treated with subcutaneous emicizumab: 1.5 mg/kg weekly (group A), 3 mg/kg every 2 weeks (group B), or 6 mg/kg every 4 weeks (group C). Pharmacokinetics, safety, and efficacy (including an intraindividual comparison of participants from a noninterventional study) were evaluated. Eighty-five participants aged <12 years were enrolled. In group A (n = 65), the annualized rate of treated bleeding events (ABRs) was 0.3 (95% confidence interval [CI], 0.17-0.50), and 77% had no treated bleeding events. Intraindividual comparison of 15 participants who previously took BPA prophylaxis showed that emicizumab prophylaxis reduced the ABR by 99% (95% CI, 97.4-99.4). In groups B (n = 10) and C (n = 10), ABRs were 0.2 (95% CI, 0.03-1.72) and 2.2 (95% CI, 0.69-6.81), respectively. The most frequent adverse events were nasopharyngitis and injection-site reactions; no thrombotic events occurred. Two of 88 participants developed antidrug antibodies (ADAs) with neutralizing potential, that is, associated with decreased emicizumab plasma concentrations: 1 experienced loss of efficacy, and, in the other, ADAs disappeared over time without intervention or breakthrough bleeding. All other participants achieved effective emicizumab plasma concentrations, regardless of the treatment regimen. Emicizumab prophylaxis has been shown to be a highly effective novel medication for children with hemophilia A and inhibitors. This trial was registered at www.clinicaltrials.gov as #NCT02795767.
© 2019 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: G.Y. has received honoraria and consulting fees from Alnylam, Bayer, Bioverativ, CSL Behring, Genentech/Roche, Grifols, Kedrion, Novo Nordisk, Shire, Spark, and uniQure, and an investigator-initiated grant award from Genentech. R.L. has consulted for CSL Behring, Novo Nordisk, Roche, Octapharma, Sobi/Biogen, Baxalta/Shire, Grifols, and Bayer. T.C. and L.Y.W. are employed by Genentech. R.S. has consulted for Bayer, Pfizer, UniQure, BioMarin, Novo Nordisk, Shire, Genentech/Roche, Spark, Octapharma, Grifols, Kedrion, and Bioverativ, and has investigator-initiated grant funding from Bioverativ, Kedrion/Grifols, Genentech, and Octapharma. J.O. has received honoraria and consulting fees from Chugai, CSL Behring, Grifols, Novo Nordisk, Octapharma, Pfizer, Roche, Sobi, and Shire, and grants from CSL Behring, Novo Nordisk, Octapharma, Pfizer, and Shire. V.J-Y. has received grants and personal fees from Novo Nordisk, Shire, Bayer, Pfizer, Grifols, Sobi, and Octapharma, and personal fees from CSL Behring and Roche. J.M. has received research grant support from Bayer, Biogen, Biomarin, CSL Behring, Novo Nordisk, Sobi, Roche, and uniQure; personal fees from Amgen, Bayer, Biotest, Biogen, Baxalta, CSL Behring, Catalyst Biosciences, Chugai, Freeline, LFB, Novo Nordisk, Roche, and Spark; and has been a member of a speaker’s bureau for Alnylam, Bayer, Biotest, Biogen, Novo Nordisk, Pfizer, Sobi, Shire, Roche, the International Society on Thrombosis and Haemostasis, and the World Federation of Hemophilia. R.K.-J. has consulted for CSL Behring, Genentech/Roche, Grifols, and Pfizer, and has received research funding from CSL Behring, Genentech/Roche, and Pfizer. M.W. has consulted for Bayer Healthcare, Bioverativ, CSL Behring, Novo Nordisk, Octapharma, Roche/Genentech, and HEMA Biologics. M.U. is employed by Roche. M.Y.D. and C.S. are employed by and hold stock with Roche. G.G.L. is employed by Genentech and holds stock with Roche. M.S. has received grants and personal fees from Shire, Bioverativ, Chugai, Novo Nordisk, and Bayer; grants from Roche, CSL Behring, and Pfizer; and personal fees from Sysmex. M.E.M. has received personal fees from Bayer, CSL Behring, Novo Nordisk, Roche, Octapharma, Pfizer, Sobi/Biogen, Bioverativ, Baxalta/Shire, Biotest, and Grifols.
Figures
References
-
- Srivastava A, Brewer AK, Mauser-Bunschoten EP, et al. ; Treatment Guidelines Working Group on Behalf of The World Federation Of Hemophilia . Guidelines for the management of hemophilia. Haemophilia. 2013;19(1):e1-e47. - PubMed
-
- Astermark J, Petrini P, Tengborn L, Schulman S, Ljung R, Berntorp E. Primary prophylaxis in severe haemophilia should be started at an early age but can be individualized. Br J Haematol. 1999;105(4):1109-1113. - PubMed
-
- Fischer K, Collins PW, Ozelo MC, Srivastava A, Young G, Blanchette VS. When and how to start prophylaxis in boys with severe hemophilia without inhibitors: communication from the SSC of the ISTH. J Thromb Haemost. 2016;14(5):1105-1109. - PubMed
-
- Warren BB, Thornhill D, Stein J, et al. Early prophylaxis provides continued joint protection in severe hemophilia A: results of the Joint Outcome Continuation Study [abstract]. Blood. 2018;132(suppl 1):382.
