

Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium
- PMID: 31699664
- PMCID: PMC8559573
- DOI: 10.1016/S1473-3099(19)30312-3
Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium
Abstract
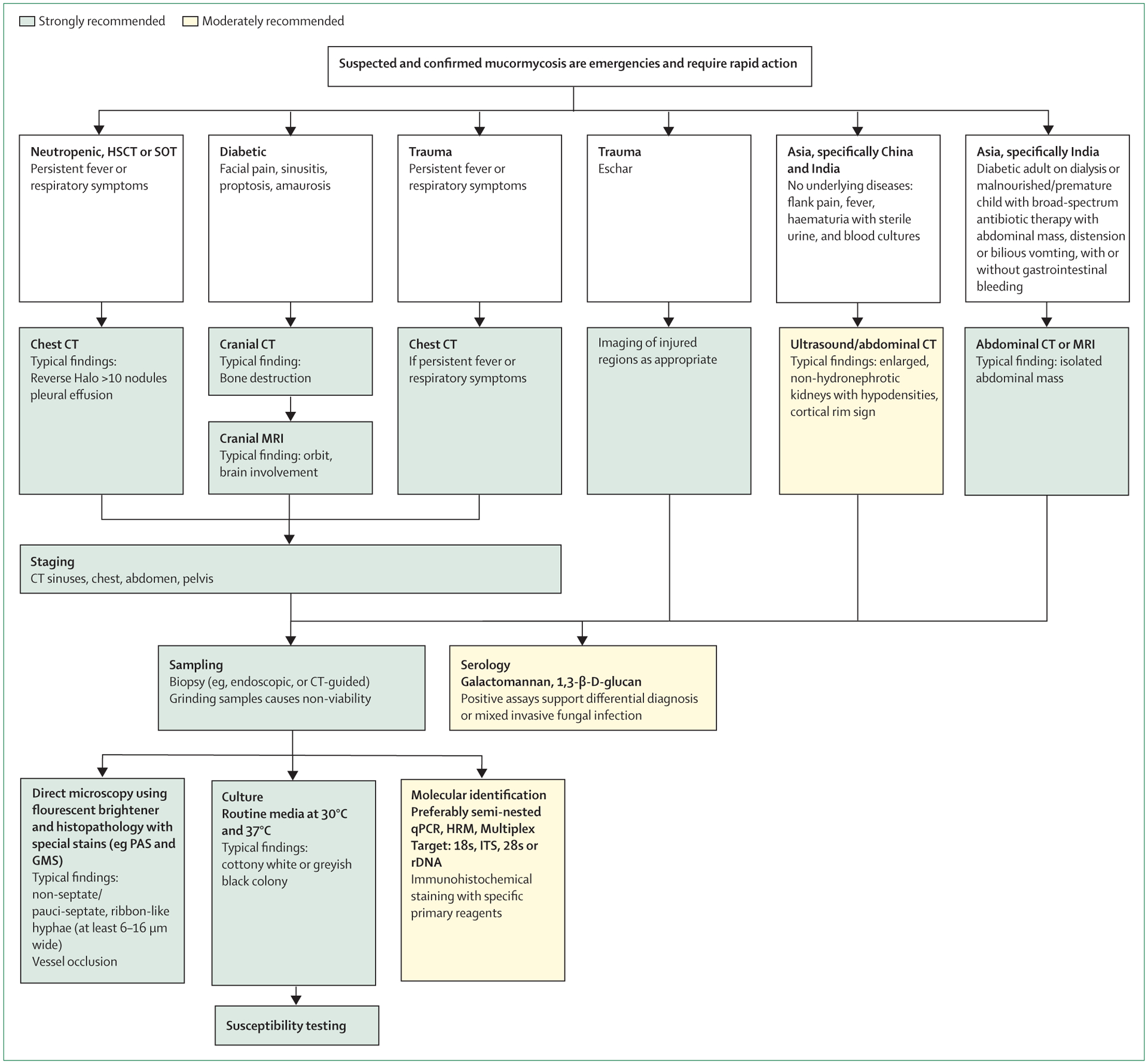
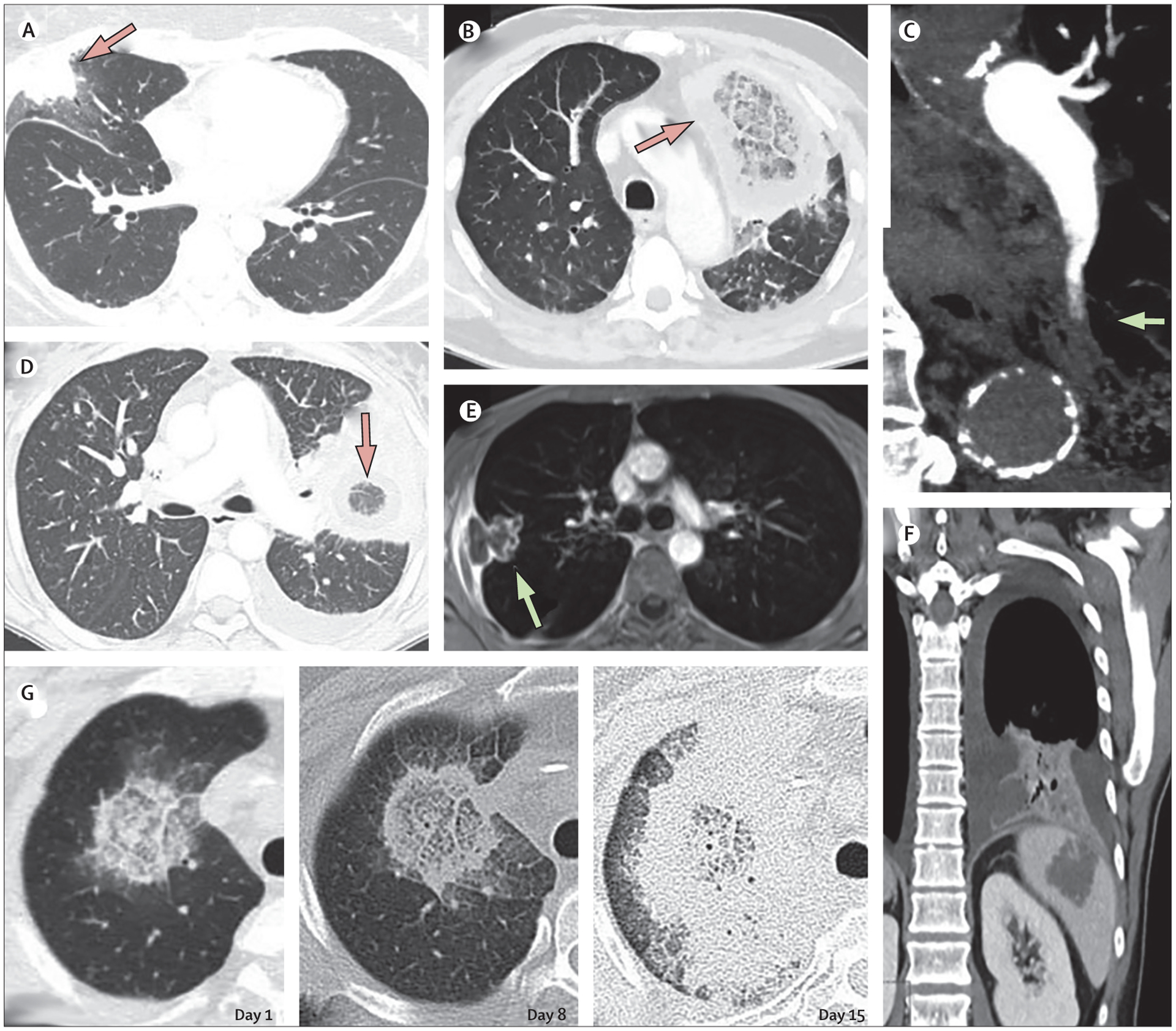
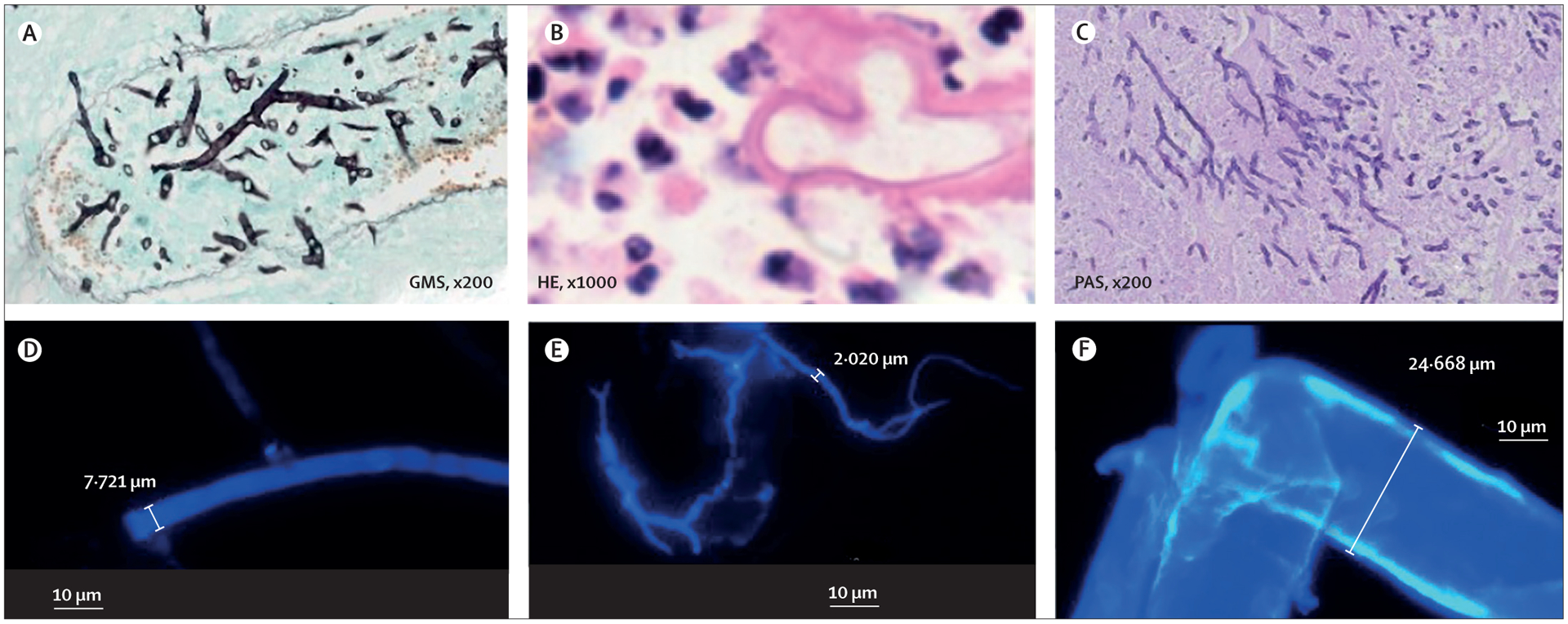
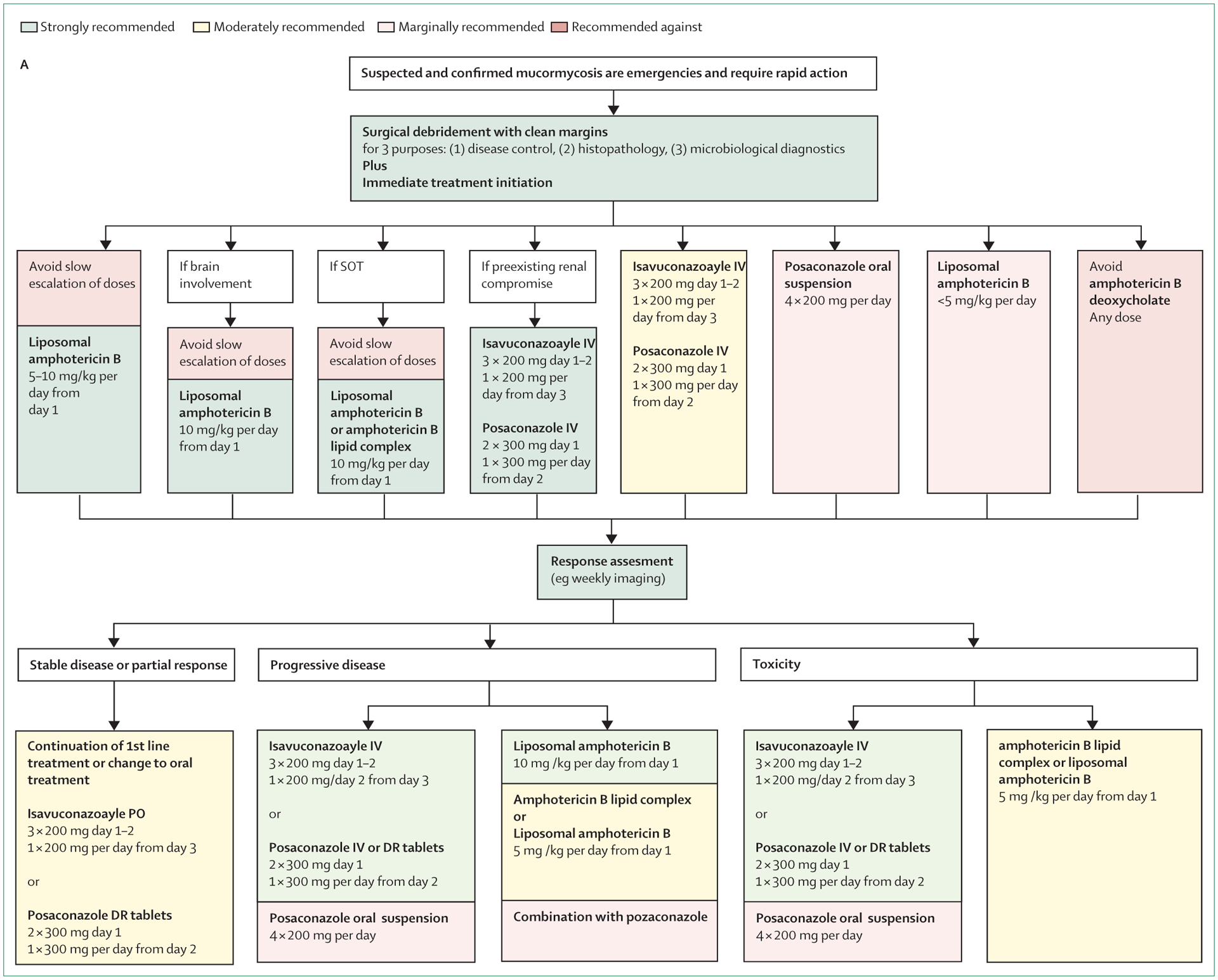
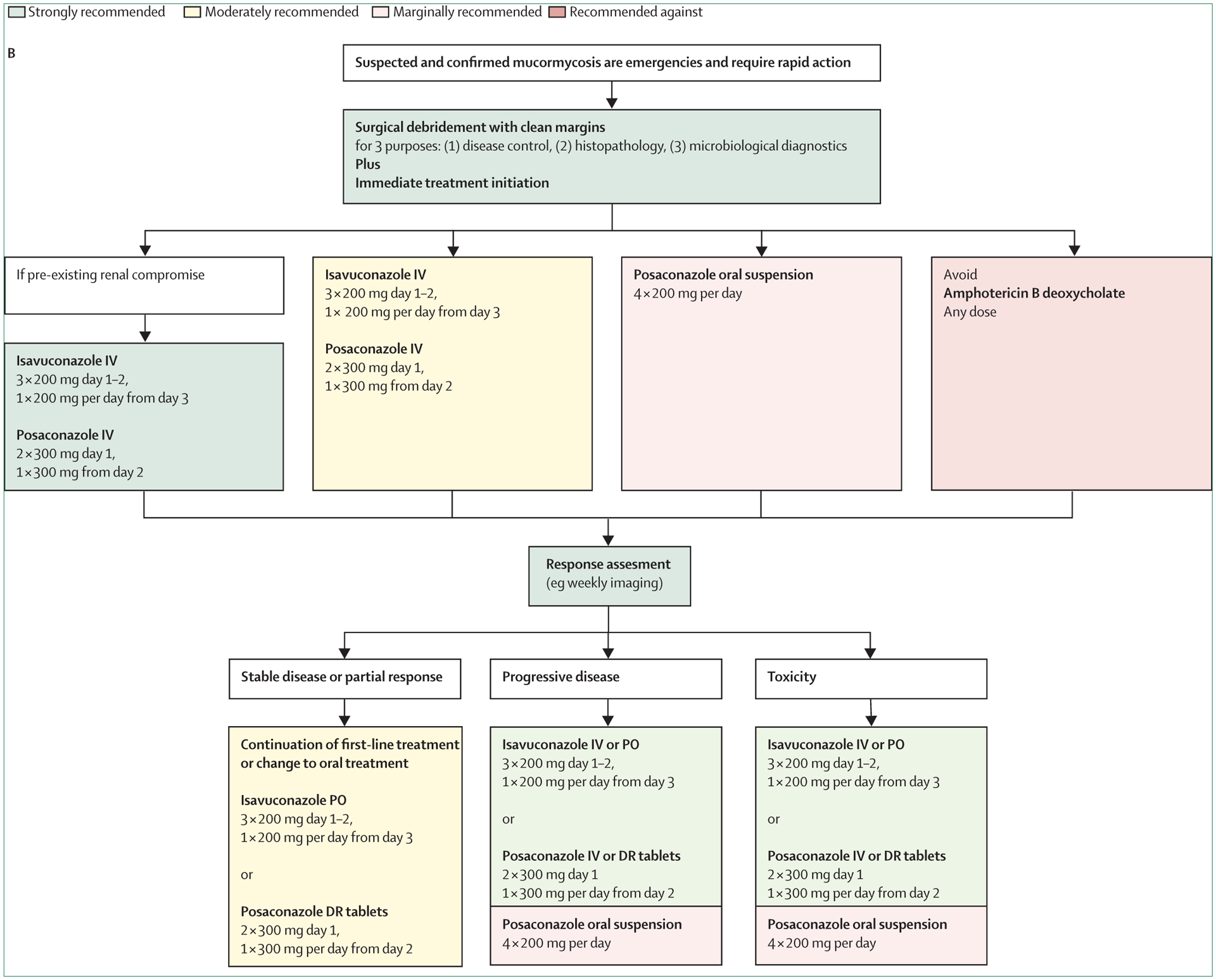
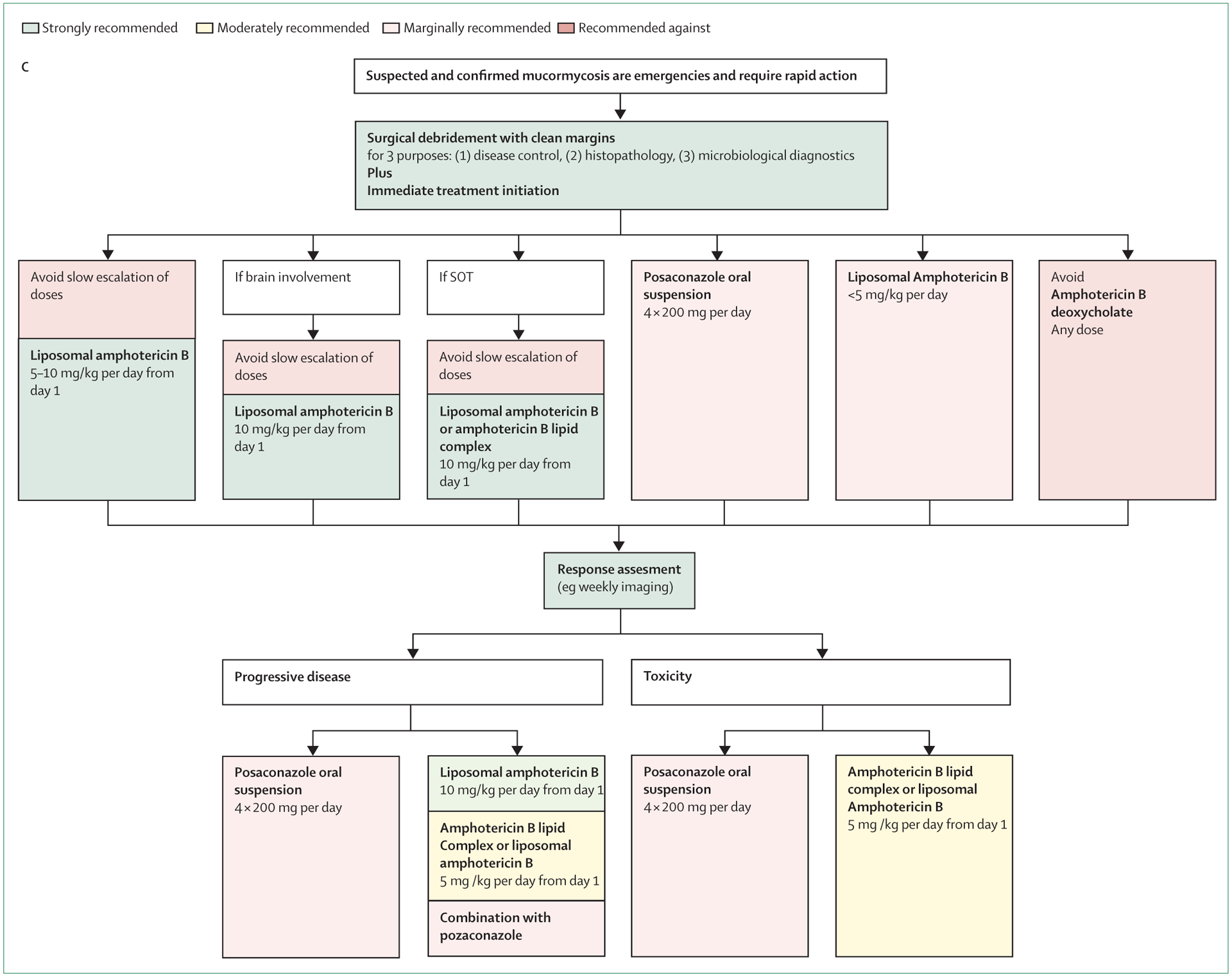
Mucormycosis is a difficult to diagnose rare disease with high morbidity and mortality. Diagnosis is often delayed, and disease tends to progress rapidly. Urgent surgical and medical intervention is lifesaving. Guidance on the complex multidisciplinary management has potential to improve prognosis, but approaches differ between health-care settings. From January, 2018, authors from 33 countries in all United Nations regions analysed the published evidence on mucormycosis management and provided consensus recommendations addressing differences between the regions of the world as part of the "One World One Guideline" initiative of the European Confederation of Medical Mycology (ECMM). Diagnostic management does not differ greatly between world regions. Upon suspicion of mucormycosis appropriate imaging is strongly recommended to document extent of disease and is followed by strongly recommended surgical intervention. First-line treatment with high-dose liposomal amphotericin B is strongly recommended, while intravenous isavuconazole and intravenous or delayed release tablet posaconazole are recommended with moderate strength. Both triazoles are strongly recommended salvage treatments. Amphotericin B deoxycholate is recommended against, because of substantial toxicity, but may be the only option in resource limited settings. Management of mucormycosis depends on recognising disease patterns and on early diagnosis. Limited availability of contemporary treatments burdens patients in low and middle income settings. Areas of uncertainty were identified and future research directions specified.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Figures

Comment in
-
Pharmacoeconomic evaluation of isavuconazole, posaconazole, and voriconazole for the treatment of invasive mold diseases in hematological patients: initial therapy prior to pathogen differential diagnosis in China.Front Public Health. 2023 Dec 19;11:1292162. doi: 10.3389/fpubh.2023.1292162. eCollection 2023. Front Public Health. 2023. PMID: 38179563 Free PMC article.
References
-
- Chamilos G, Lewis RE, Kontoyiannis DP. Delaying amphotericin B-based frontline therapy significantly increases mortality among patients with hematologic malignancy who have zygomycosis. Clin Infect Dis 2008; 47: 503–09. - PubMed
-
- Vaughan C, Bartolo A, Vallabh N, Leong SC. A meta-analysis of survival factors in rhino-orbital-cerebral mucormycosis—has anything changed in the past 20 years? Clin Otolaryngol 2018; 43: 1454–64. - PubMed
-
- Sun HY, Singh N. Mucormycosis: its contemporary face and management strategies. Lancet Infect Dis 2011; 11: 301–11. - PubMed
-
- Kung HC, Huang PY, Chen WT, et al. 2016 guidelines for the use of antifungal agents in patients with invasive fungal diseases in Taiwan. J Microbiol Immunol Infect 2018; 51: 1–17. - PubMed
