

Trends in Bronchiolitis Hospitalizations in the United States: 2000-2016
- PMID: 31699829
- PMCID: PMC6889950
- DOI: 10.1542/peds.2019-2614
Trends in Bronchiolitis Hospitalizations in the United States: 2000-2016
Abstract
Objectives: To investigate the temporal trend in the national incidence of bronchiolitis hospitalizations, their characteristics, inpatient resource use, and hospital cost from 2000 through 2016.
Methods: We performed a serial, cross-sectional analysis of nationally representative samples (the 2000, 2003, 2006, 2009, 2012, and 2016 Kids' Inpatient Databases) of children (age <2 years) hospitalized for bronchiolitis. We identified all children hospitalized with bronchiolitis by using International Classification of Diseases, Ninth Revision, Clinical Modification 466.1 and International Classification of Diseases, 10th Revision, Clinical Modification J21. Complex chronic conditions were defined by the pediatric complex chronic conditions classification by using inpatient data. The primary outcomes were the incidence of bronchiolitis hospitalizations, mechanical ventilation use, and hospital direct cost. We examined the trends accounting for sampling weights.
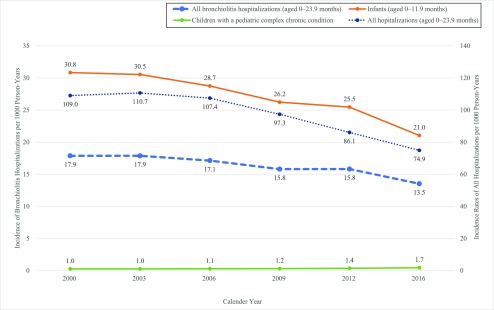
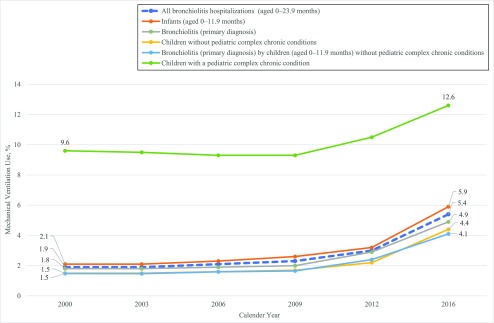
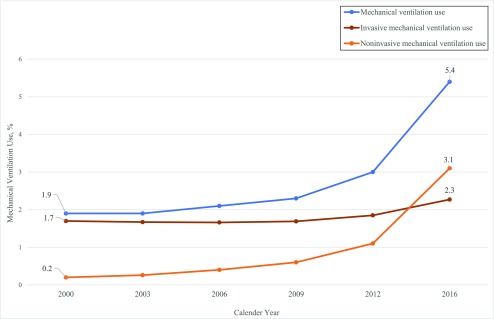
Results: From 2000 to 2016, the incidence of bronchiolitis hospitalization decreased from 17.9 to 13.5 per 1000 person-years in US children (25% decrease; P trend < .001). In contrast, the proportion of bronchiolitis hospitalizations among overall hospitalizations increased from 16% to 18% (P trend < .001). There was an increase in the proportion of children with a complex chronic condition (6%-13%; 117% increase), hospitalization to children's hospital (15%-29%; 93% increase), and mechanical ventilation use (2%-5%; 184% increase; all P trend < .001). Likewise, the hospital cost increased from $449 million to $734 million (63% increase) nationally (with an increase in geometric mean of cost per hospitalization [from $3267 to $4086; 25% increase; P trend < .001] adjusted for inflation) from 2003 to 2016.
Conclusions: From 2000 through 2016, the incidence of bronchiolitis hospitalizations among US children declined. In contrast, mechanical ventilation use and nationwide hospital direct cost substantially increased.
Copyright © 2019 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
References
-
- American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis Diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774–1793 - PubMed
-
- Glezen WP, Taber LH, Frank AL, Kasel JA. Risk of primary infection and reinfection with respiratory syncytial virus. Am J Dis Child. 1986;140(6):543–546 - PubMed
-
- Hasegawa K, Mansbach JM, Camargo CA Jr. Infectious pathogens and bronchiolitis outcomes. Expert Rev Anti Infect Ther. 2014;12(7):817–828 - PubMed
-
- Christakis DA, Cowan CA, Garrison MM, et al. . Variation in inpatient diagnostic testing and management of bronchiolitis. Pediatrics. 2005;115(4):878–884 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
