

Glomerular filtration rate by differing measures, albuminuria and prediction of cardiovascular disease, mortality and end-stage kidney disease
- PMID: 31700174
- PMCID: PMC6858876
- DOI: 10.1038/s41591-019-0627-8
Glomerular filtration rate by differing measures, albuminuria and prediction of cardiovascular disease, mortality and end-stage kidney disease
Erratum in
-
Author Correction: Glomerular filtration rate by differing measures, albuminuria and prediction of cardiovascular disease, mortality and end-stage kidney disease.Nat Med. 2020 Aug;26(8):1308. doi: 10.1038/s41591-020-0996-z. Nat Med. 2020. PMID: 32669718
Abstract
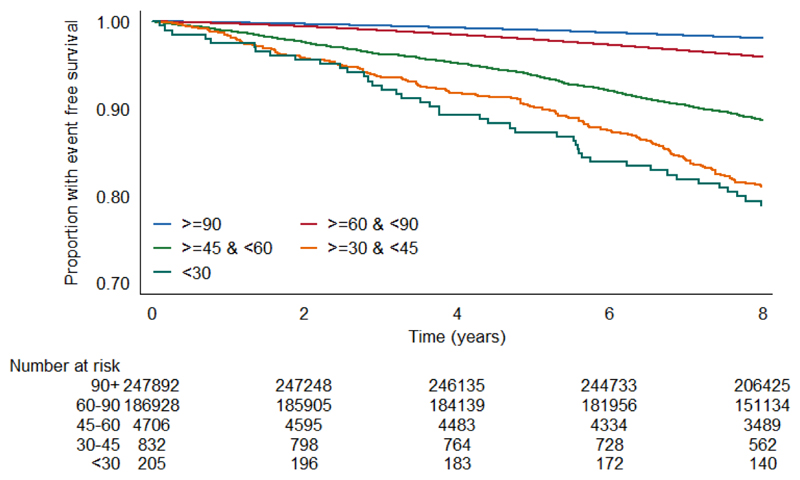
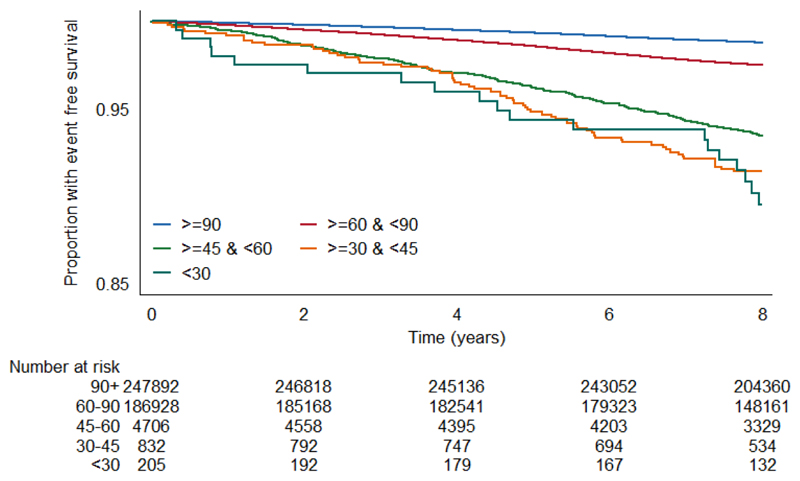
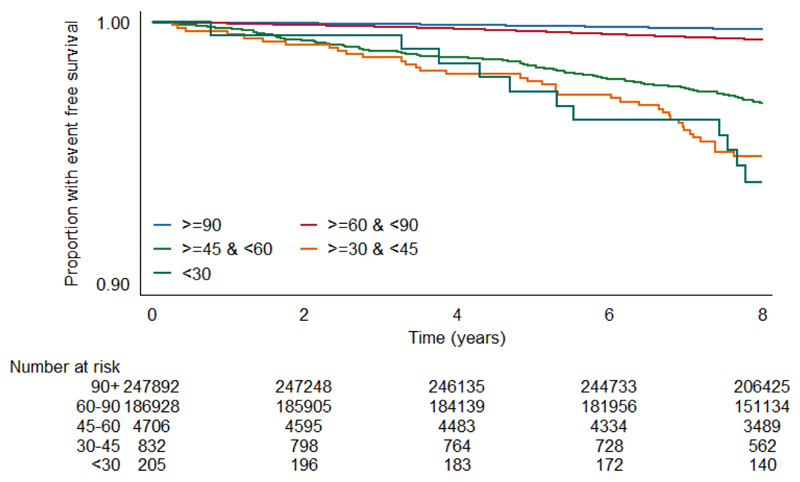
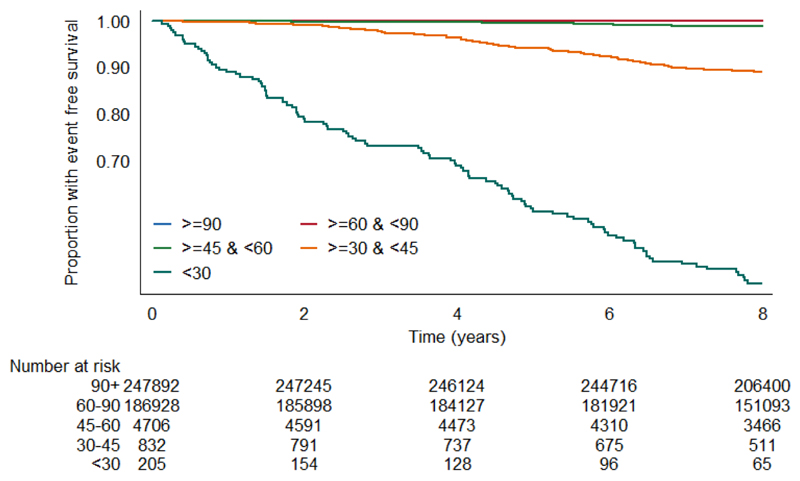
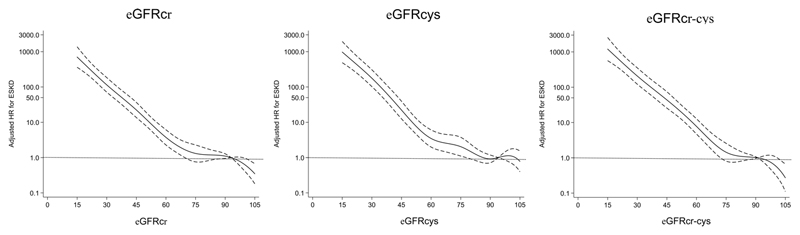
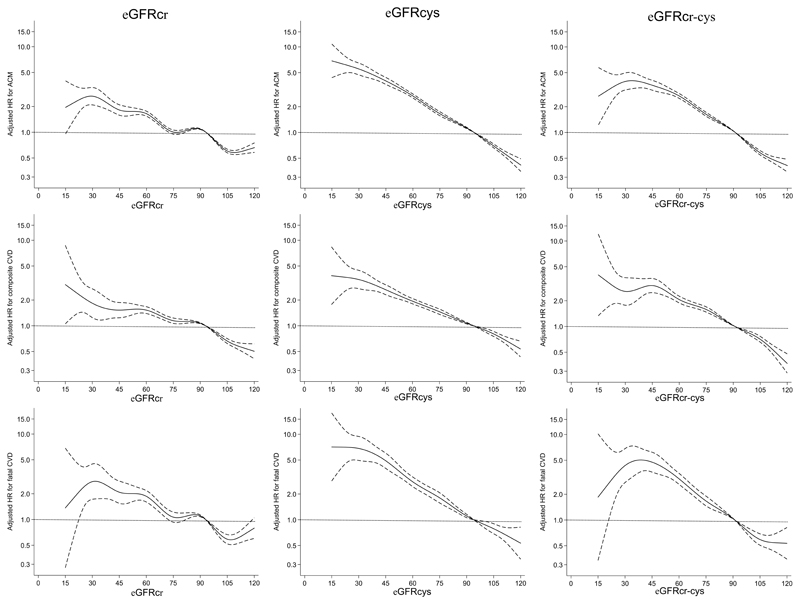
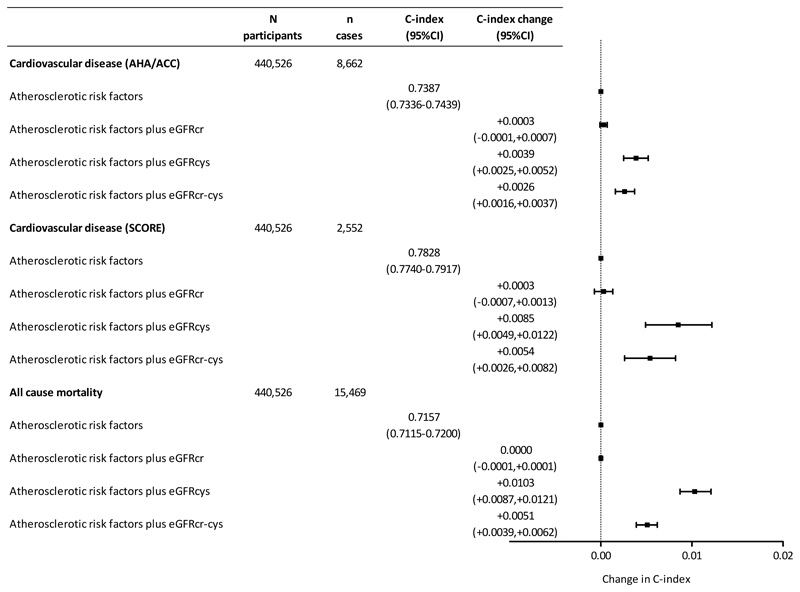
Chronic kidney disease is common in the general population and associated with excess cardiovascular disease (CVD), but kidney function does not feature in current CVD risk-prediction models. We tested three formulae for estimated glomerular filtration rate (eGFR) to determine which was the most clinically informative for predicting CVD and mortality. Using data from 440,526 participants from UK Biobank, eGFR was calculated using serum creatinine, cystatin C (eGFRcys) and creatinine-cystatin C. Associations of each eGFR with CVD outcome and mortality were compared using Cox models and adjusting for atherosclerotic risk factors (per relevant risk scores), and the predictive utility was determined by the C-statistic and categorical net reclassification index. We show that eGFRcys is most strongly associated with CVD and mortality, and, along with albuminuria, adds predictive discrimination to current CVD risk scores, whilst traditional creatinine-based measures are weakly associated with risk. Clinicians should consider measuring eGFRcys as part of cardiovascular risk assessment.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu C. Chronic Kidney Disease and the Risks of Death, Cardiovascular Events, and Hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
