

Head and neck cancer management and cancer stem cells implication
- PMID: 31700218
- PMCID: PMC6823822
- DOI: 10.1016/j.sdentj.2019.05.010
Head and neck cancer management and cancer stem cells implication
Abstract
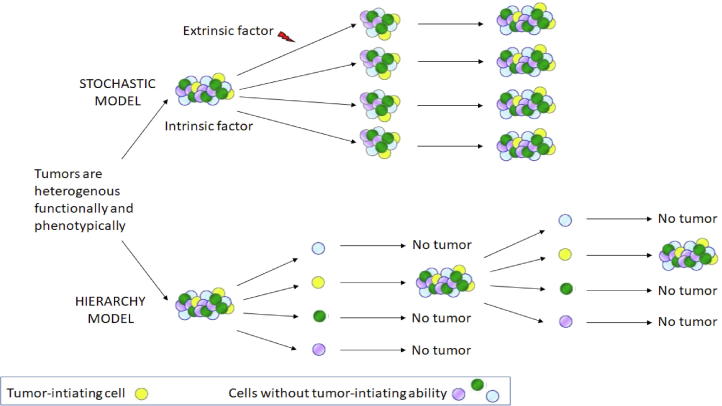
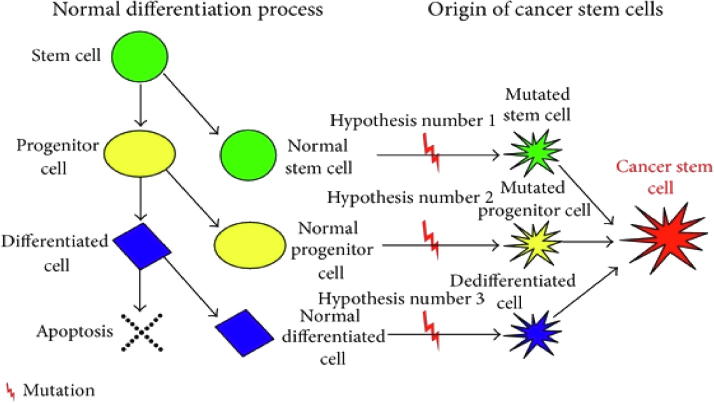
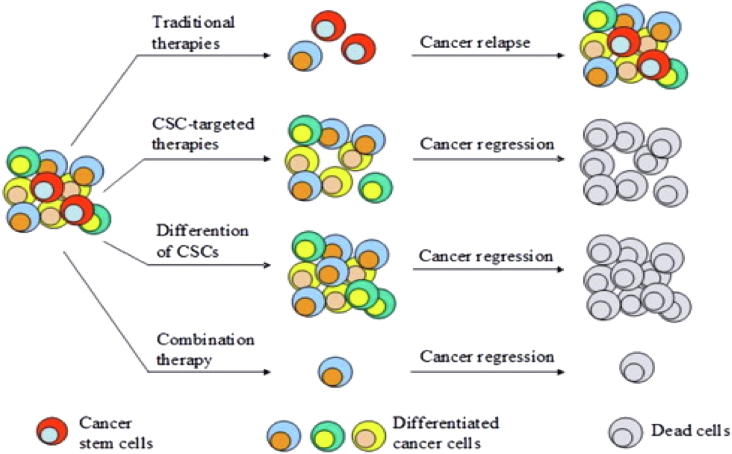
Head and neck squamous cell carcinomas (HNSCCs) arise in the mucosal linings of the upper aerodigestive tract and are heterogeneous in nature. Risk factors for HNSCCs are smoking, excessive alcohol consumption, and the human papilloma virus. Conventional treatments are surgery, radiotherapy, chemotherapy, or a combined modality; however, no international standard mode of therapy exists. In contrast to the conventional model of clonal evolution in tumor development, there is a newly proposed theory based on the activity of cancer stem cells (CSCs) as the model for carcinogenesis. This "CSC hypothesis" may explain the high mortality rate, low response to treatments, and tendency to develop multiple tumors for HNSCC patients. We review current knowledge on HNSCC etiology and treatment, with a focus on CSCs, including their origins, identifications, and effects on therapeutic options.
Keywords: ABC, ATP-binding cassette transporters; ATC, amplifying transitory cell; Antineoplastic agents; BMI-1, B cell-specific Moloney murine leukemia virus integration site 1; Cancer stem cells; Cancer treatment; Carcinoma; EGFR, epidermal growth factor receptor; HIFs, hypoxia-inducible factors; Head and neck cancer; MDR1, Multidrug Resistance Protein 1; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; PI3K, phosphatidylinositol-4,5-bisphosphate 3-kinase; Squamous cell; TKIs, tyrosine kinase inhibitors.
© 2019 The Authors.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures
References
-
- Abdul-Hamid G., Saeed N.M., Al-Kahiry W., Shukry S. Pattern of head and neck cancer in Yemen. Gulf J.Oncolog. 2010;(7):21–24. - PubMed
-
- Abollo-Jimenez F., Jimenez R., Cobaleda C. Physiological cellular reprogramming and cancer. Semin. Cancer Biol. 2010;20(2):98–106. - PubMed
-
- Acharya S., Ekalaksananan T., Vatanasapt P., Loyha K., Phusingha P., Promthet S. Association of Epstein-Barr virus infection with oral squamous cell carcinoma in a case-control study. J. Oral Pathol. Med. 2015;44(4):252–257. - PubMed
-
- El-Naggar Adel K., Chan John K.C., Grandis Jennifer R., Takata Takashi, Slootweg Pieter J. International Agency for Research on Cancer; 2017. WHO Classification of Head and Neck Tumours.
-
- Adelstein D.J., Li Y., Adams G.L., Wagner H., Jr., Kish J.A., Ensley J.F. An intergroup phase III comparison of standard radiation therapy and two schedules of concurrent chemoradiotherapy in patients with unresectable squamous cell head and neck cancer. J. Clin. Oncol. 2003;21(1):92–98. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
