

Is it Safe and Cost Saving to Defer the CD4+ Cell Count Monitoring in Stable Patients on Art with More than 350 or 500 cells/μl?
- PMID: 31700588
- PMCID: PMC6827605
- DOI: 10.4084/MJHID.2019.063
Is it Safe and Cost Saving to Defer the CD4+ Cell Count Monitoring in Stable Patients on Art with More than 350 or 500 cells/μl?
Abstract
Background: CD4+ lymphocyte cell count represents the main immunological marker used to monitor HIV infection. However, frequent monitoring may be unnecessary, could cause anxiety to the patient as well as burdening healthcare with extra expenses.
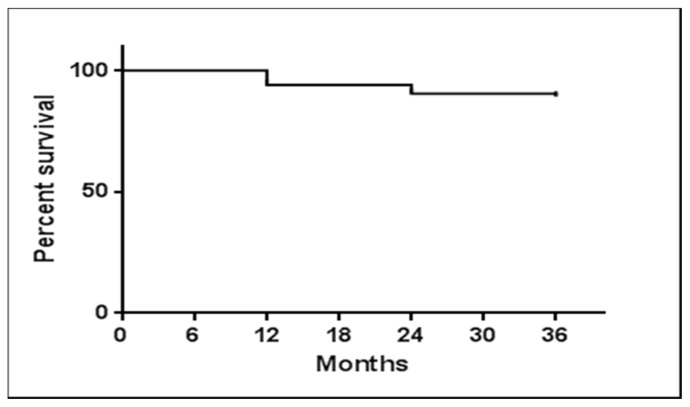
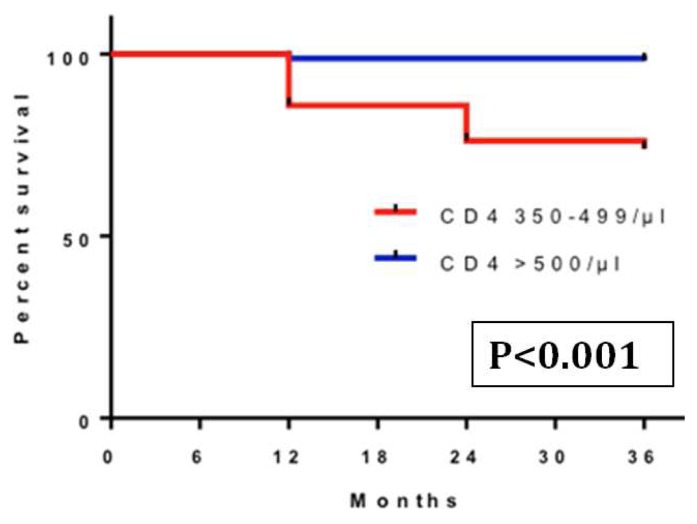
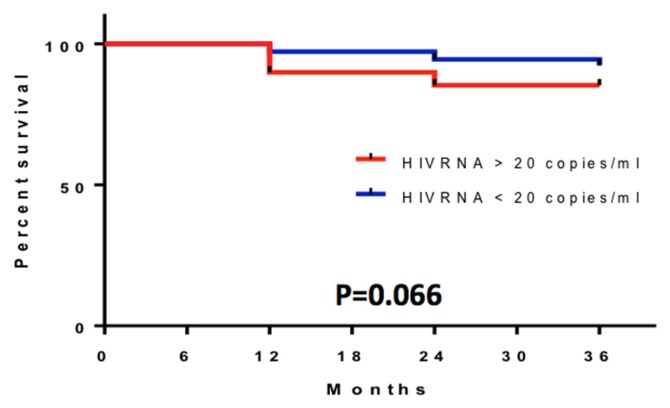
Objectives and methods: A two-step retrospective (safety and cost-saving) analysis was performed to evaluate the probability of maintaining a safe number of more than 350 CD4+ cells/μl in HIV-positive subjects under treatment during a three-year follow up and secondarily to estimate in real life the cost of the CD4+ determinations in a 3 years period, speculating on possible cost-saving strategies. The safety analyses was conducted with Kaplan-Meyer method considering: 1) all patients independently from their viral load (VL); 2) patients with 500 > CD4+ ≥ 350 cells/μl versus (vs) CD4+ ≥ 500 cells/μl at baseline; 3) patients with VL < 20 copies/ml vs VL > 20 copies/ml. The cost-saving analysis measuring the costs of CD4+ determinations was calculated from April 1, 2013, to March 31, 2016.
Results: In the safety analysis, 253 subjects were enrolled. The median CD4+ count was 623 (489-805) cells/μl. Subjects maintaining ≥ 350 cells/μl in the first, second, and third year were respectively 238 (94.1%), 229 (90.5%), and 226 (89.3%), independently from VL. Within subjects with ≥ 350 CD4+/μl vs. ≥ 500 CD4+/μl at baseline, those who maintained ≥ 350 cells/μl until the third year were respectively 241 (95.3%) and 158 (98.1%). The probability of maintaining these values in the third year was 89.3% for those who had CD4+ ≥ 350/μl at baseline and 98.1% for those who had CD4+ ≥ 500/μl. This probability was around 90% vs. 99% for subjects with HIV-RNA above or below 20 copies/ml. In the real-life cost saving analysis, we evaluated subjects with a stable value or more than 500 CD4+ (respectively 343, 364 and 383 in the first, second and third period). We observed mean value of about two determinations patient/year (2.41 in 2013/2014; 2.32 in 2014/2015; 2.18 in 2015/2016), with a significant decrease between the first and the last period (p<0.001). The mean cost patient/year was €101.51 in the first year, €97.61 in the second, €92.00 in the third (p<0,001). Assuming to extend these procedures to all our patients with stable CD4+ cells/μl and monitoring CD4+ cell count once in a year, we were able to obtain an overall saving of €19,152/year.
Conclusions: A very high percentage of subjects maintained a high and safe number of CD4+ cells (>350 cells/μl) during a three-year follow-up. It could be possible to save up to 66% of the costs by reducing the number of CD4+ count determinations in a year, to have other favorable consequences as well, releasing new resources for patient management.
Keywords: CD4 monitoring; HIV; Saving analysis; Saving cost.
Conflict of interest statement
Competing interests: The authors declare no conflict of Interest.
Figures
References
-
- UNAIDS. Fact sheet. 2018. 2017 Global HIV Statistics.
-
- Antinori A, et al. Italian guidelines for the use of antiretroviral agents and the diagnostic-clinical management of HIV-1 infected persons. Update 2016. New Microbiol. 2017 - PubMed
-
- EACS. European AIDS Clinical Society Guidelines Version 9.0 October 2017. European AIDS Clinical Society (EACS); 2017.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous