

Biochemical Control in Acromegaly With Multimodality Therapies: Outcomes From a Pituitary Center and Changes Over Time
- PMID: 31701145
- PMCID: PMC8660161
- DOI: 10.1210/clinem/dgz187
Biochemical Control in Acromegaly With Multimodality Therapies: Outcomes From a Pituitary Center and Changes Over Time
Abstract
Purpose: To determine the prevalence of insulin-like growth factor-1 (IGF-1) normalization with long-term multimodality therapy in a pituitary center and to assess changes over time.
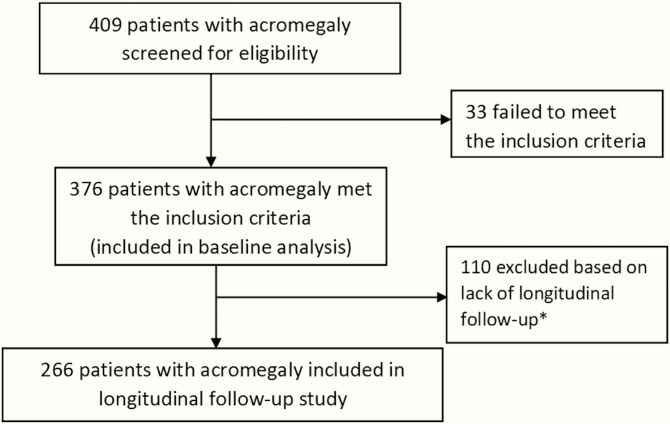
Methods: Patients with acromegaly (N = 409), with ≥1 year of data after surgery and at least 2 subsequent clinic visits were included in long-term analysis (N = 266). Biochemical data, clinical characteristics, and therapeutic interventions were reviewed retrospectively.
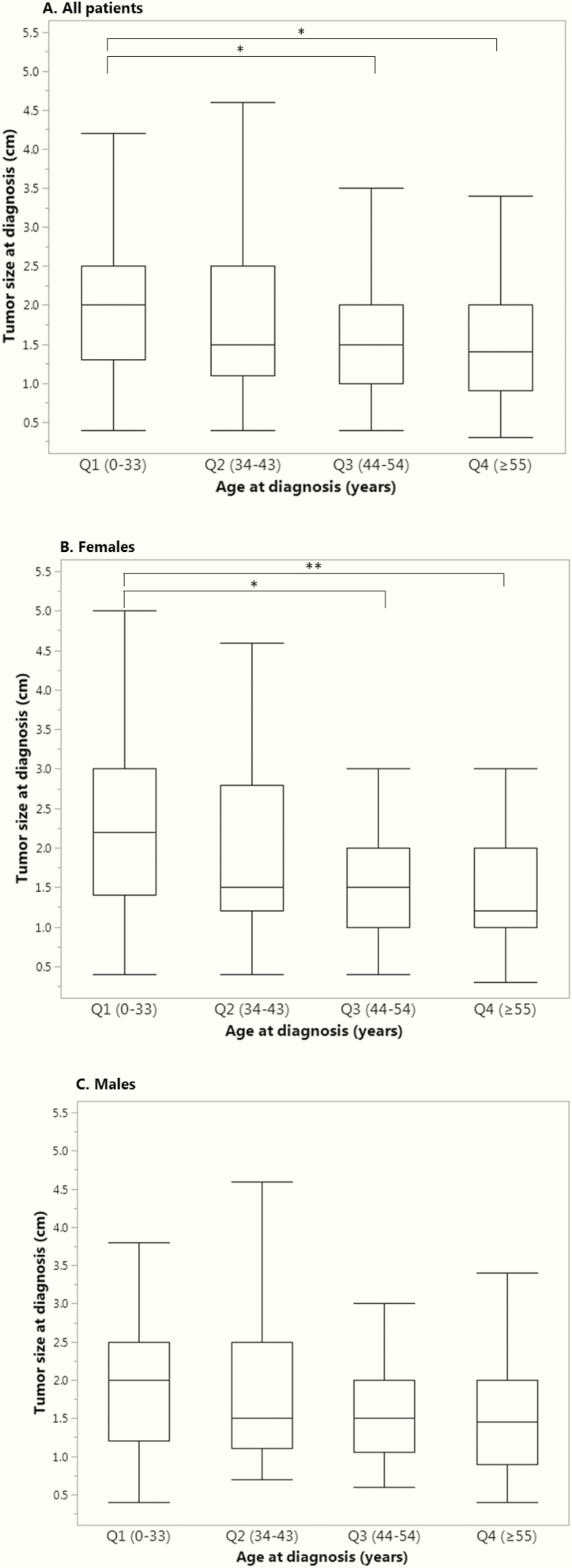
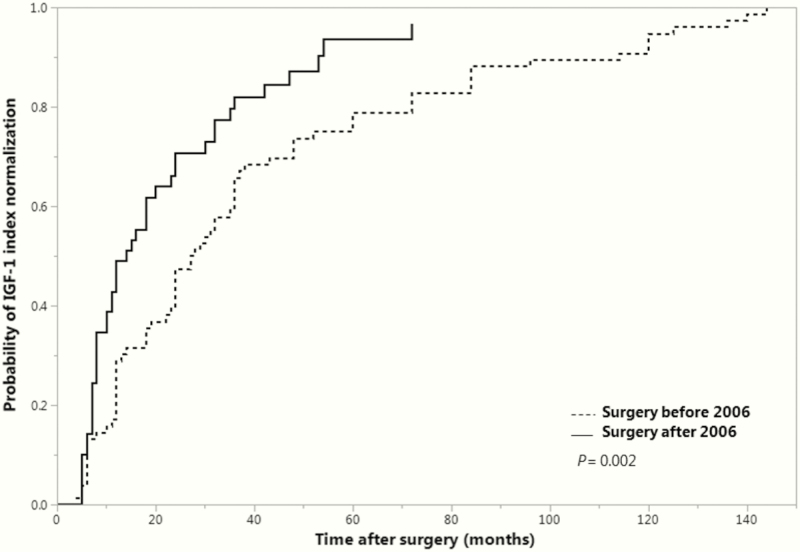
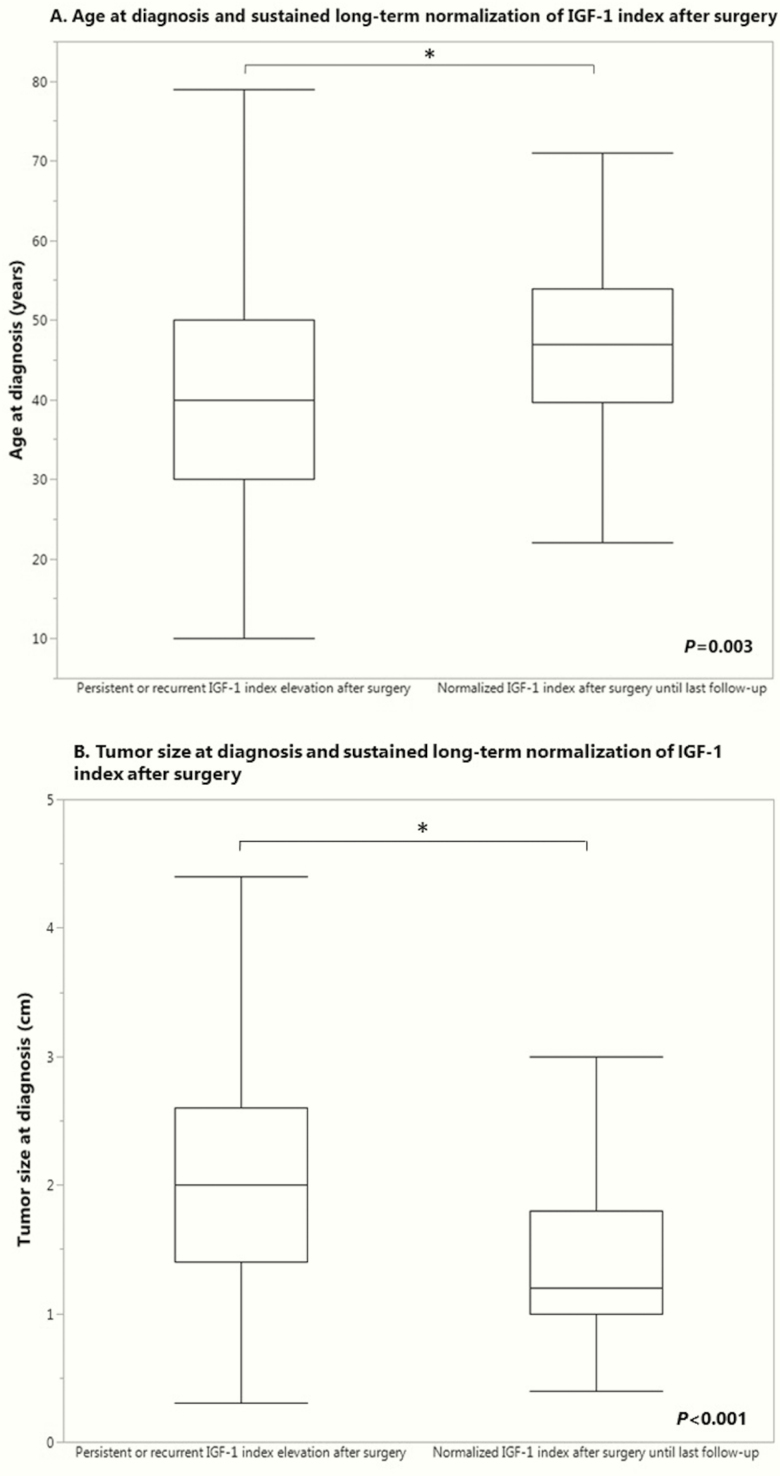
Results: At diagnosis, mean [standard deviation] age was 43.4 [14.3] years, body mass index was 28.5 (24.9-32.1) kg/m2 (median, interquartile range), serum IGF-1 index (IGF-1 level/upper limit of normal) was 2.3 [1.7-3.1], and 80.5% had macroadenomas. Patients with transsphenoidal surgery after 2006 were older [46.6 ± 14.3 vs 40.0 ± 13.4 years; P < 0.001]. Age and tumor size correlated inversely. Overall (N = 266), 93.2% achieved a normal IGF-1 level during 9.9 [5.0-15.0] years with multimodality therapy. The interval to first normal IGF-1 level following failed surgical remission was shorter after 2006: 14.0 (95% confidence interval, 10.0-20.0) versus 27.5 (22.0-36.0) months (P = 0.002). Radiation therapy and second surgery were rarer after 2006: 28 (22%) versus 62 (47.0%); P < 0.001 and 12 (9.4%) versus 28 (21.2%); P = 0.010, respectively. Age at diagnosis increased over time periods, possibly reflecting increased detection of acromegaly in older patients with milder disease. Male gender, older age, smaller tumor and lower IGF-1 index at diagnosis predicted long-term sustained IGF-1 control after surgery without adjuvant therapies.
Conclusion: The vast majority of patients with acromegaly can be biochemically controlled with multimodality therapy in the current era. Radiotherapy and repeat pituitary surgery became less frequently utilized over time. Long-term postoperative IGF-1 control without use of adjuvant therapies has improved.
Keywords: Acromegaly; IGF-1; medical therapy; pituitary center; pituitary surgery; radiation therapy.
© Endocrine Society 2019. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Colao A, Grasso LFS, Giustina A, et al. . Nat Rev Dis Primers. 2019;5(1):20. - PubMed
-
- Katznelson L, Laws ER Jr, Melmed S, et al. ; Endocrine Society . Acromegaly: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(11):3933–3951. - PubMed
-
- Fernandez-Rodriguez E, Casanueva FF, Bernabeu I. Update on prognostic factors in acromegaly: Is a risk score possible? Pituitary. 2015;18(3):431–440. - PubMed
-
- Dal J, Feldt-Rasmussen U, Andersen M, et al. . Acromegaly incidence, prevalence, complications and long-term prognosis: a nationwide cohort study. Eur J Endocrinol. 2016;175(3):181–190. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
