

One-stage Debridement via Oblique Lateral Interbody Fusion Corridor Combined with Posterior Pedicle Screw Fixation in Treating Spontaneous Lumbar Infectious Spondylodiscitis: A Case Series
- PMID: 31701667
- PMCID: PMC6904647
- DOI: 10.1111/os.12562
One-stage Debridement via Oblique Lateral Interbody Fusion Corridor Combined with Posterior Pedicle Screw Fixation in Treating Spontaneous Lumbar Infectious Spondylodiscitis: A Case Series
Abstract
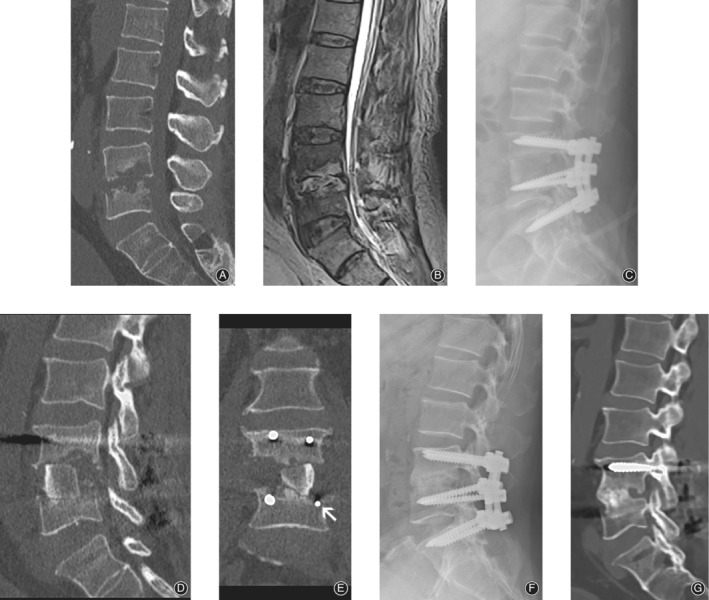
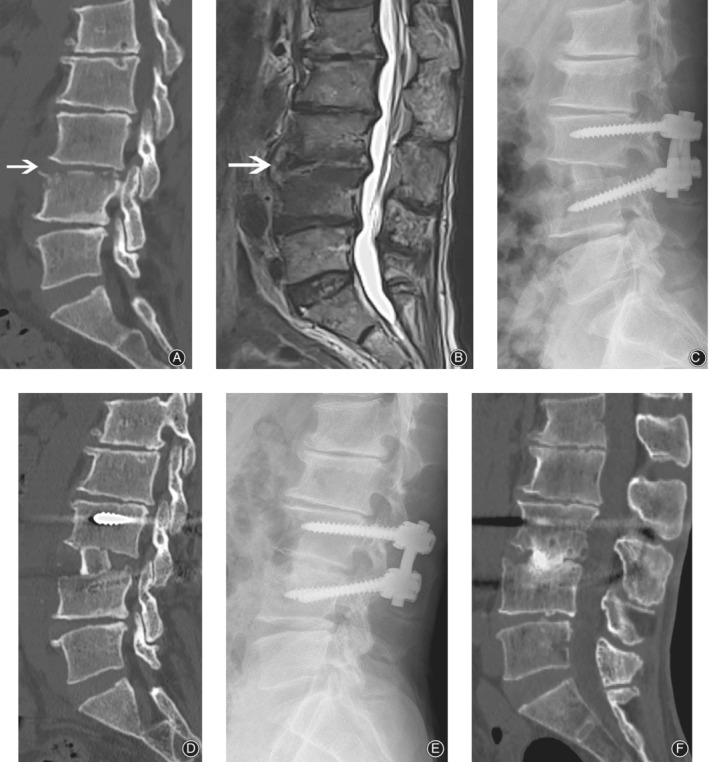
Objective: Surgery is indicated when antibiotic treatment fails in pyogenic spondylodiscitis, which is caused by pathogens such as the Staphylococcus species. The aim of the present study was to investigate the efficacy and safety of the oblique lateral interbody fusion (OLIF) corridor approach combined with posterior pedicle screw fixation for treating pyogenic spondylodiscitis.
Methods: This was a retrospective case series study. A total of 11 patients with an average age of 60.7 years (range, 40-70 years; 10 males and 1 females) with lumbar pyogenic spondylodiscitis who underwent single-stage debridement and reconstruction using the OLIF corridor combined with posterior pedicle screw fixation were recruited in our study from June 2016 to July 2017. All patients had single-level pyogenic spondylodiscitis between T12 and L5 . The baseline data, perioperative outcomes (operative time, intra-operative blood loss, and intra-operative complication), postoperative laboratory tests (erythrocyte sedimentation rate [ESR], C-reactive protein [CRP], white blood count [WBC], and tissue culture results), long-term complications (recurrence, fixation failure, and bony non-fusion rates), and duration of antibiotic administration were reviewed. Outcomes evaluated using a variety of scales including visual analog scale (VAS) score and Oswestry disability index (ODI), were compared pre-operatively and post-operatively.
Results: The mean follow-up period of time was 18.3 months. The average operative time and intra-operative blood loss were 217.0 ± 91.91 min and 220.9 ± 166.10 mL, respectively. There were no intra-operative complications, except in 1 patient who encountered somatosensory evoked potentials changes and 1 patient who had motor evoked potentials changes, both without post-surgery neurological deficits. Causative organisms were identified in 4 patients: Staphylococcus aureus in 1 patient and Streptococcus in 3 patients. At approximately 8.8 weeks after surgery, WBC, CRP, and ESR had returned to normal levels. All patients were pain free with no recurring infection. There was no fixation failure during follow up. Solid bony fusions were observed in all cases within 6 months. At the final follow up, the mean VAS (0.6 ± 0.69) and ODI (14.4 ± 4.27) were significantly lower than those before surgery (P < 0.05).
Conclusion: One-stage debridement with autogenous iliac bone graft through the OLIF corridor combined with posterior pedicle screw fixation is effective and safe for single-level spontaneous lumbar pyogenic spondylodiscitis after antibiotic treatment fails.
Keywords: Anterior lumbar interbody fusion; Extremal lateral lumbar interbody fusion; Lumbar pyogenic spondylodiscitis; Oblique lateral interbody fusion corridor; Vascular and nerve injury.
© 2019 The Authors. Orthopaedic Surgery published by Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures

References
-
- Kehrer M, Pedersen C, Jensen TG, Lassen AT. Increasing incidence of pyogenic spondylodiscitis: a 14‐year population‐based study. J Infect, 2014, 68: 313–320. - PubMed
-
- Sundararaj GD, Babu N, Amritanand R, et al Treatment of haematogenous pyogenic vertebral osteomyelitis by single‐stage anterior debridement, grafting of the defect and posterior instrumentation. J Bone Joint Surg Br, 2007, 89: 1201–1205. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
