

Patients With Primary Aldosteronism Respond to Unilateral Adrenalectomy With Long-Term Reduction in Salt Intake
- PMID: 31702016
- PMCID: PMC7010311
- DOI: 10.1210/clinem/dgz051
Patients With Primary Aldosteronism Respond to Unilateral Adrenalectomy With Long-Term Reduction in Salt Intake
Abstract
Context: High dietary salt intake is known to aggravate arterial hypertension. This effect could be of particular relevance in the setting of primary aldosteronism (PA), which is associated with cardiovascular damage independent of blood pressure levels. The aim of this study was to determine the impact of therapy on salt intake in PA patients.
Patients and methods: A total of 148 consecutive PA patients (66 with unilateral and 82 with bilateral PA) from the database of the German Conn's Registry were included. Salt intake was quantified by 24-hour urinary sodium excretion before and after initiation of PA treatment.
Study design: Observational longitudinal cohort study.
Setting: Tertiary care hospital.
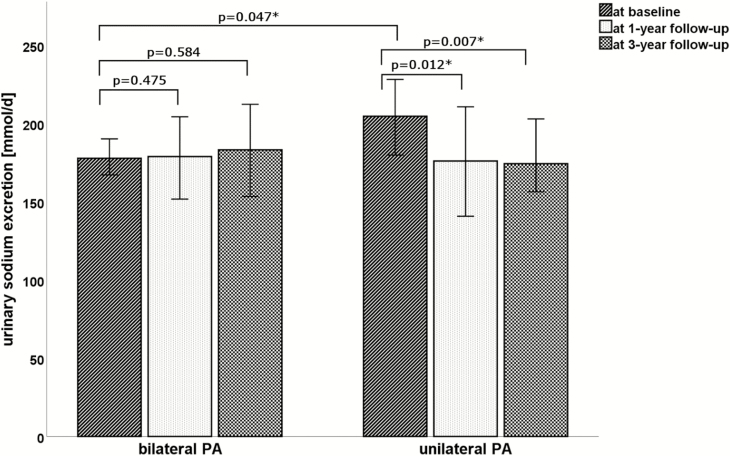
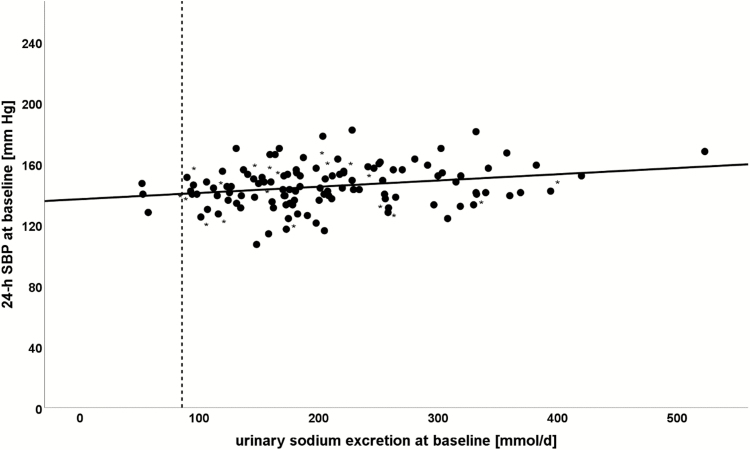
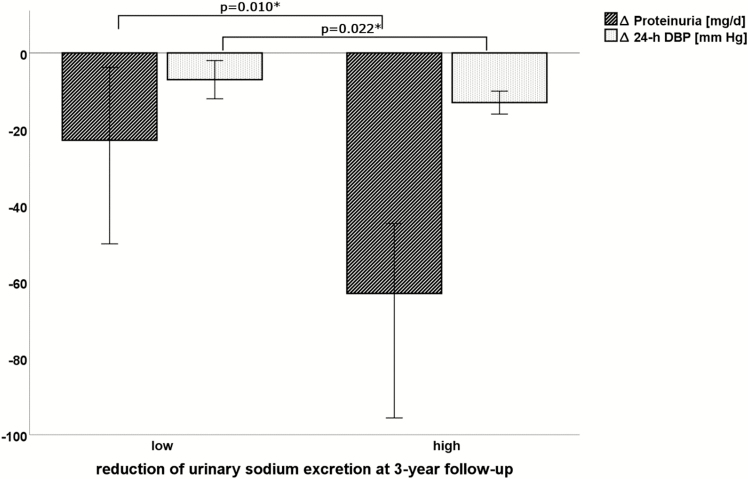
Results: At baseline, unilateral PA patients had a significantly higher urinary sodium excretion than patients with bilateral disease (205 vs 178 mmol/d, P = 0.047). Higher urinary sodium excretion correlated with an increased cardiovascular risk profile including proteinuria, impaired lipid, and glucose metabolism and was associated with higher daily doses of antihypertensive drugs to achieve blood pressure control. In unilateral disease, urinary sodium excretion dropped spontaneously to 176 mmol/d (P = 0.012) 1 year after unilateral adrenalectomy and remained low at 3 years of follow-up (174 mmol/d). In contrast, treatment with mineralocorticoid receptor antagonists (MRA) in bilateral PA patients was not associated with a significant change in urinary sodium excretion at follow-up (179 mmol/d vs 183 mmol/d).
Conclusion: PA patients consuming a high-salt diet, estimated based on urinary sodium excretion, respond to adrenalectomy with a significant reduction of salt intake, in contrast to MRA treatment.
Keywords: adrenalectomy; cardiovascular risk; hypertension; primary aldosteronism; salt intake; sodium excretion.
© Endocrine Society 2019.
Figures
Similar articles
-
Dietary Salt Intake Is a Determinant of Cardiac Changes After Treatment of Primary Aldosteronism: A Prospective Study.Hypertension. 2016 Jul;68(1):204-12. doi: 10.1161/HYPERTENSIONAHA.116.07615. Epub 2016 May 31. Hypertension. 2016. PMID: 27245179
-
Post-saline infusion test aldosterone levels indicate severity and outcome in primary aldosteronism.Eur J Endocrinol. 2015 Apr;172(4):443-50. doi: 10.1530/EJE-14-1013. Epub 2015 Jan 28. Eur J Endocrinol. 2015. PMID: 25630564 Clinical Trial.
-
Salt intake in mineralocorticoid receptor antagonist-treated primary aldosteronism: foe or ally?Hormones (Athens). 2020 Jun;19(2):223-232. doi: 10.1007/s42000-019-00167-9. Epub 2019 Dec 21. Hormones (Athens). 2020. PMID: 31863347
-
Outcomes of drug-based and surgical treatments for primary aldosteronism.Adv Chronic Kidney Dis. 2015 May;22(3):196-203. doi: 10.1053/j.ackd.2014.10.003. Adv Chronic Kidney Dis. 2015. PMID: 25908468 Review.
-
Salt Appetite and its Effects on Cardiovascular Risk in Primary Aldosteronism.Horm Metab Res. 2020 Jun;52(6):386-393. doi: 10.1055/a-1116-2407. Epub 2020 Apr 6. Horm Metab Res. 2020. PMID: 32252107 Review.
Cited by
-
Control of sodium appetite by hindbrain aldosterone-sensitive neurons.Mol Cell Endocrinol. 2024 Oct 1;592:112323. doi: 10.1016/j.mce.2024.112323. Epub 2024 Jun 26. Mol Cell Endocrinol. 2024. PMID: 38936597 Review.
-
Aldosterone-induced salt appetite requires HSD2 neurons.JCI Insight. 2024 Dec 6;9(23):e175087. doi: 10.1172/jci.insight.175087. JCI Insight. 2024. PMID: 39446486 Free PMC article.
-
Sex-dependent modulation of T and NK cells and gut microbiome by low sodium diet in patients with primary aldosteronism.Front Immunol. 2024 Dec 19;15:1428054. doi: 10.3389/fimmu.2024.1428054. eCollection 2024. Front Immunol. 2024. PMID: 39749333 Free PMC article. Clinical Trial.
-
Biomarkers to Guide Medical Therapy in Primary Aldosteronism.Endocr Rev. 2024 Jan 4;45(1):69-94. doi: 10.1210/endrev/bnad024. Endocr Rev. 2024. PMID: 37439256 Free PMC article. Review.
-
Effects of a low-sodium diet in patients with idiopathic hyperaldosteronism: a randomized controlled trial.Front Endocrinol (Lausanne). 2023 Apr 19;14:1124479. doi: 10.3389/fendo.2023.1124479. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37152926 Free PMC article. Clinical Trial.
References
-
- Zhao L, Stamler J, Yan LL, Zhou B, Wu Y, Liu K, Daviglus ML, Dennis BH, Elliott P, Ueshima H, Yang J, Zhu L, Guo D; INTERMAP Research Group . Blood pressure differences between northern and southern Chinese: role of dietary factors: the International Study on Macronutrients and Blood Pressure. Hypertension. 2004;43(6):1332–1337. - PMC - PubMed
-
- Stolarz-Skrzypek K, Kuznetsova T, Thijs L, Tikhonoff V, Seidlerová J, Richart T, Jin Y, Olszanecka A, Malyutina S, Casiglia E, Filipovský J, Kawecka-Jaszcz K, Nikitin Y, Staessen JA; European Project on Genes in Hypertension (EPOGH) Investigators . Fatal and nonfatal outcomes, incidence of hypertension, and blood pressure changes in relation to urinary sodium excretion. JAMA. 2011;305(17):1777–1785. - PubMed
