

Effects of epinephrine for out-of-hospital cardiac arrest: A systematic review and meta-analysis of randomized controlled trials
- PMID: 31702610
- PMCID: PMC6855610
- DOI: 10.1097/MD.0000000000017502
Effects of epinephrine for out-of-hospital cardiac arrest: A systematic review and meta-analysis of randomized controlled trials
Abstract
Aim: Our objective is to assess the effects of epinephrine for out of hospital cardiac arrest.
Background: Cardiac arrest was the most serious medical incidents with an estimated incidence in the United States of 95.7 per 100,000 person years. Though epinephrine improved coronary and cerebral perfusion, improving a return of spontaneous circulation, potentially harmful effects on the heart lead to greater myocardial oxygen demand. Concerns about the effect of epinephrine for out-of-hospital cardiac arrest were controversial and called for a higher argument to determine whether the effects of epinephrine is safe and effective for shor and long terms outcomes.
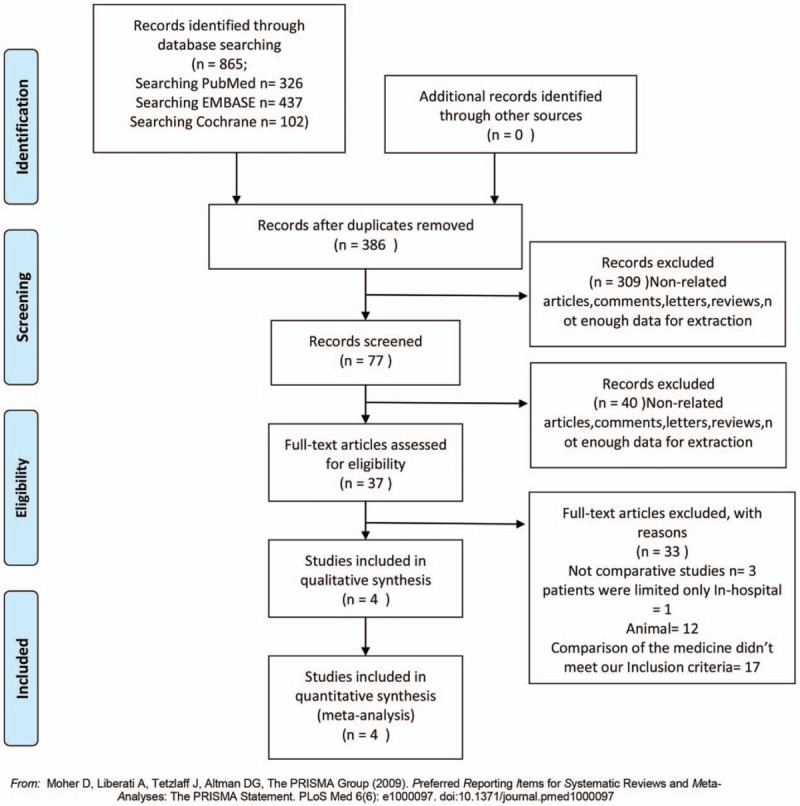
Method: Searching databases consist of all kinds of searching tools, such as Medline, the Cochrane Library, Embase, PubMed, etc. All the included studies should meet our demand of this meta-analysis. In the all interest outcomes blow we take the full advantage of STATA to assess, the main measure is Risk Ratio (RR) with 95% confidence, the publication bias are assessed by Egger Test.
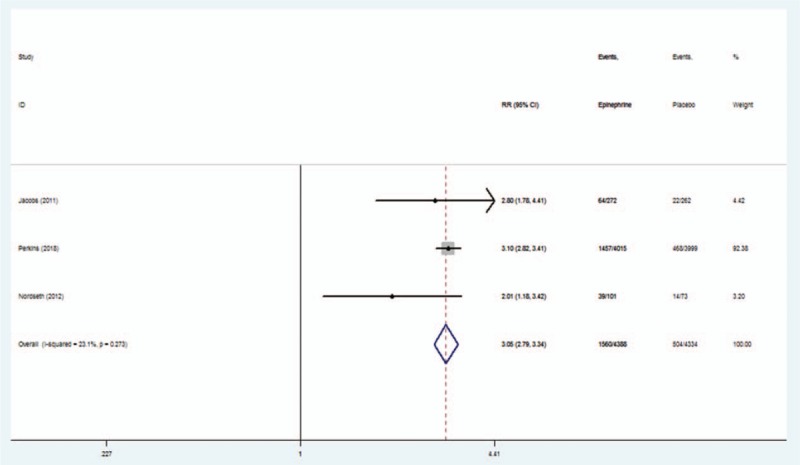
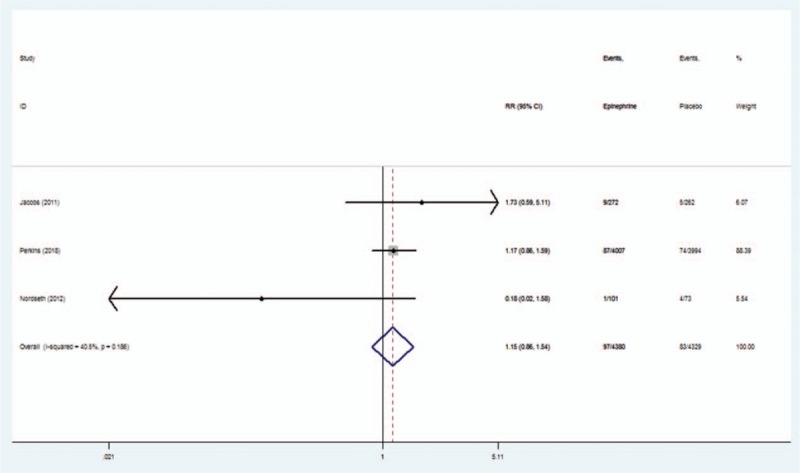
Result: In current systematic review and meta-analysis of randomized trials investigating epinephrine for out of hospital cardiac arrest, we found that epinephrine was associated with a significantly higher likelihood of ROSC (RR = 3.05, I = 23.1%, P = .0001) and survival to hospital discharge (RR = 1.40, I = 36.3%, P = .008) compared with non-adrenaline administration. Conversely, epinephrine did not increase CPC 1 or 2 (RR = 1.15, I = 40.5%, P = .340) and hospital admission (RR = 2.07, I = 88.2%, P = .0001).
Conclusion: In conclusion, in this systematic review and meta-analysis involving studies, the use of epinephrine resulted in a significantly higher likelihood of survival to hospital discharge and ROSC than the non-epinephrine administration, but, there was no significant between group difference in the rate of a favorable neurologic outcome.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures




References
-
- Ornato JP, Becker LB, Weisfeldt ML, et al. Cardiac arrest and resuscitation: an opportunity to align research prioritization and public health need. Circulation 2010;122:1876–9. - PubMed
-
- Soar J, Callaway CW, Aibiki M, et al. Part 4: Advanced life support: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation 2015;95:e71–120. - PubMed
-
- Pearson JW, Redding JS. The role of epinephrine in cardiac resuscitation. Anesth Analg 1963;42:599–606. - PubMed
-
- Pearson JW, Redding JS. Epinephrine in cardiac resuscitation. Am Heart J 1963;66:210–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
