

Development of Risk Prediction Equations for Incident Chronic Kidney Disease
- PMID: 31703124
- PMCID: PMC6865298
- DOI: 10.1001/jama.2019.17379
Development of Risk Prediction Equations for Incident Chronic Kidney Disease
Abstract
Importance: Early identification of individuals at elevated risk of developing chronic kidney disease (CKD) could improve clinical care through enhanced surveillance and better management of underlying health conditions.
Objective: To develop assessment tools to identify individuals at increased risk of CKD, defined by reduced estimated glomerular filtration rate (eGFR).
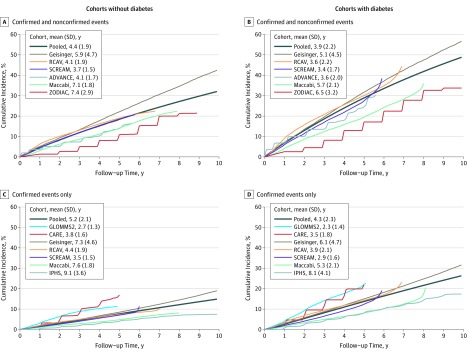
Design, setting, and participants: Individual-level data analysis of 34 multinational cohorts from the CKD Prognosis Consortium including 5 222 711 individuals from 28 countries. Data were collected from April 1970 through January 2017. A 2-stage analysis was performed, with each study first analyzed individually and summarized overall using a weighted average. Because clinical variables were often differentially available by diabetes status, models were developed separately for participants with diabetes and without diabetes. Discrimination and calibration were also tested in 9 external cohorts (n = 2 253 540).
Exposures: Demographic and clinical factors.
Main outcomes and measures: Incident eGFR of less than 60 mL/min/1.73 m2.
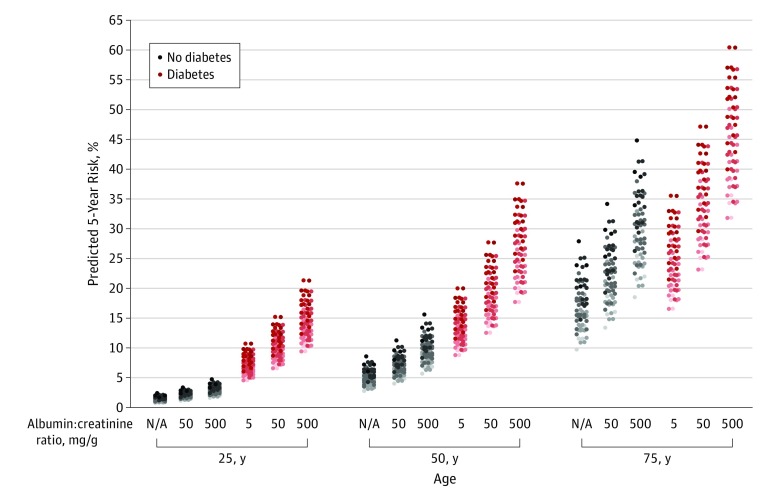
Results: Among 4 441 084 participants without diabetes (mean age, 54 years, 38% women), 660 856 incident cases (14.9%) of reduced eGFR occurred during a mean follow-up of 4.2 years. Of 781 627 participants with diabetes (mean age, 62 years, 13% women), 313 646 incident cases (40%) occurred during a mean follow-up of 3.9 years. Equations for the 5-year risk of reduced eGFR included age, sex, race/ethnicity, eGFR, history of cardiovascular disease, ever smoker, hypertension, body mass index, and albuminuria concentration. For participants with diabetes, the models also included diabetes medications, hemoglobin A1c, and the interaction between the 2. The risk equations had a median C statistic for the 5-year predicted probability of 0.845 (interquartile range [IQR], 0.789-0.890) in the cohorts without diabetes and 0.801 (IQR, 0.750-0.819) in the cohorts with diabetes. Calibration analysis showed that 9 of 13 study populations (69%) had a slope of observed to predicted risk between 0.80 and 1.25. Discrimination was similar in 18 study populations in 9 external validation cohorts; calibration showed that 16 of 18 (89%) had a slope of observed to predicted risk between 0.80 and 1.25.
Conclusions and relevance: Equations for predicting risk of incident chronic kidney disease developed from more than 5 million individuals from 34 multinational cohorts demonstrated high discrimination and variable calibration in diverse populations. Further study is needed to determine whether use of these equations to identify individuals at risk of developing chronic kidney disease will improve clinical care and patient outcomes.
Conflict of interest statement
Figures
Comment in
-
Predicting Risk of Kidney Disease: Is Risk-Based Kidney Care on the Horizon?JAMA. 2019 Dec 3;322(21):2079-2081. doi: 10.1001/jama.2019.17378. JAMA. 2019. PMID: 31703118 Free PMC article. No abstract available.
-
Can We Assess Interventions to Prevent Kidney Disease?Am J Kidney Dis. 2020 Aug;76(2):292-294. doi: 10.1053/j.ajkd.2020.01.014. Epub 2020 May 20. Am J Kidney Dis. 2020. PMID: 32444069 No abstract available.
References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789-1858. doi:10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- GBD 2017 Causes of Death Collaborators Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736-1788. doi:10.1016/S0140-6736(18)32203-7 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
