

Severe traumatic valgus instability of the elbow: pathoanatomy and outcomes of primary operation
- PMID: 31703693
- PMCID: PMC6839221
- DOI: 10.1186/s13018-019-1374-8
Severe traumatic valgus instability of the elbow: pathoanatomy and outcomes of primary operation
Abstract
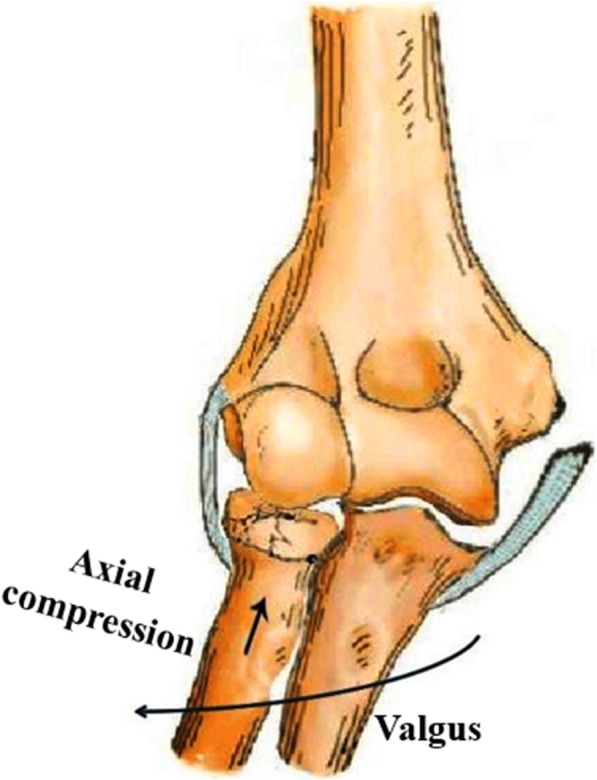
Background: The objective of the study was to depict the pathoanatomy of traumatic valgus instability of the elbow and to report clinical outcomes of primary operation.
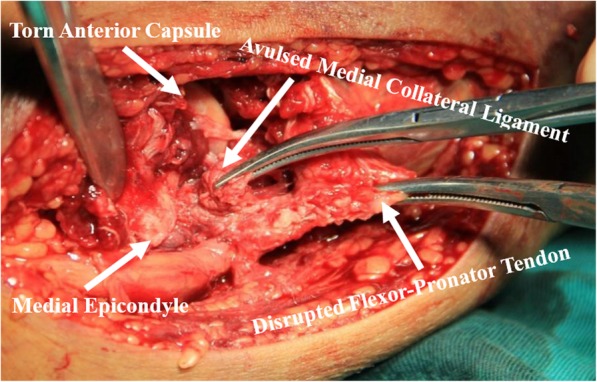
Methods: Thirty-one patients presented with traumatic valgus instability of the elbow without dislocation. Thirty-one patients underwent surgical intervention of radial head fractures (28 open reduction and internal fixation and 3 radial head resection) and anatomical repair of the anterior bundle of medial collateral ligament (AMCL) with suture anchors. Twenty patients with disruption of the flexor-pronator tendon (FPT) and 14 patients with tears of the anterior capsule had primary repair of the FPT and anterior capsule simultaneously. Clinical outcomes were evaluated with the Mayo Elbow Performance Score (MEPS), modified hospital for special surgery assessment scale (HSS), and Disabilities of the Arm, Shoulder, and Hand (DASH) score.
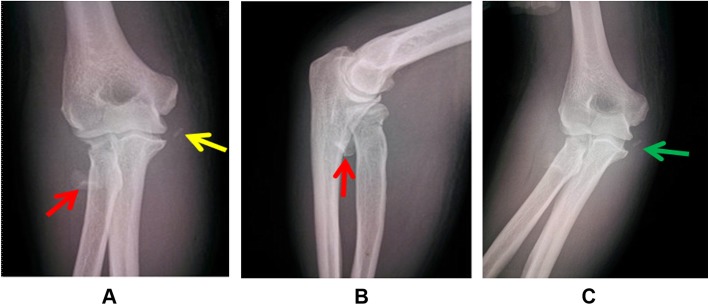
Results: The median follow-up was 37.3 months (range, 15-53 months). Radial head fractures and complete avulsion of the medial collateral ligament (MCL) from its humeral footprint were confirmed in all patients intraoperatively. Intraoperative findings indicated disruption of the FPT in 20 patients and tears of the anterior capsule in 14 patients. Twenty-nine of 31 patients returned to previous activity and work levels within 6 months after surgery. The MEPS, modified HSS, and DASH score were 94 ± 4, 91 ± 5, and 8 ± 2 at the latest follow-up.
Conclusions: Radial head fractures with avulsion of the MCL can lead to severe valgus instability of the elbow. Primary operation to repair these disrupted structures, especially repair of the AMCL, can effectively restore valgus stability.
Keywords: Elbow; Flexor-pronator tendon; Instability; Medial collateral ligament; Radial head; Valgus.
Conflict of interest statement
Not applicable. No conflict of interest exists in the submission of this manuscript, and the manuscript is approved by all authors for publication.
The authors declare that they have no competing interests.
Figures



Similar articles
-
Acute severe valgus instability without elbow dislocation.J Shoulder Elbow Surg. 2015 Aug;24(8):e212-7. doi: 10.1016/j.jse.2015.04.009. Epub 2015 Jun 23. J Shoulder Elbow Surg. 2015. PMID: 26116204
-
Traumatic valgus instability of the elbow: pathoanatomy and results of direct repair. Surgical technique.J Bone Joint Surg Am. 2009 Oct 1;91 Suppl 2:191-9. doi: 10.2106/JBJS.I.00426. J Bone Joint Surg Am. 2009. PMID: 19805583
-
Traumatic valgus instability of the elbow: pathoanatomy and results of direct repair.J Bone Joint Surg Am. 2008 Nov;90(11):2416-22. doi: 10.2106/JBJS.G.01448. J Bone Joint Surg Am. 2008. PMID: 18978410
-
Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. Surgical technique.J Bone Joint Surg Am. 2005 Mar;87 Suppl 1(Pt 1):22-32. doi: 10.2106/JBJS.D.02933. J Bone Joint Surg Am. 2005. PMID: 15743844 Review.
-
[Operative treatment of terrible triad injury of the elbow : Open reduction and internal fixation].Oper Orthop Traumatol. 2017 Apr;29(2):125-137. doi: 10.1007/s00064-017-0489-5. Epub 2017 Mar 17. Oper Orthop Traumatol. 2017. PMID: 28314869 Review. German.
Cited by
-
Role of the transverse ligament of the ulnar collateral ligament of the elbow: a biomechanical study.JSES Int. 2021 Mar 23;5(3):549-553. doi: 10.1016/j.jseint.2021.01.009. eCollection 2021 May. JSES Int. 2021. PMID: 34136869 Free PMC article.
-
Operative treatment of Mason Type III radial head fractures - A comparative analysis using PROMIS.J Orthop. 2024 Mar 30;52:129-132. doi: 10.1016/j.jor.2024.03.031. eCollection 2024 Jun. J Orthop. 2024. PMID: 38596621 Free PMC article.
References
-
- Charalambous CP, Stanley JK, Siddique I, Powell E, Ramamurthy C, Gagey O. Radial head fracture in the medial collateral ligament deficient elbow; biomechanical comparison of fixation, replacement and excision in human cadavers. Injury. 2006;37:849–853. doi: 10.1016/j.injury.2006.04.125. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
