

Immunogenicity and safety of an adjuvanted inactivated polio vaccine, IPV-Al, compared to standard IPV: A phase 3 observer-blinded, randomised, controlled trial in infants vaccinated at 6, 10, 14 weeks and 9 months of age
- PMID: 31703934
- PMCID: PMC6983932
- DOI: 10.1016/j.vaccine.2019.10.064
Immunogenicity and safety of an adjuvanted inactivated polio vaccine, IPV-Al, compared to standard IPV: A phase 3 observer-blinded, randomised, controlled trial in infants vaccinated at 6, 10, 14 weeks and 9 months of age
Abstract
Background: A dose-sparing inactivated polio vaccine (IPV-Al), obtained by adsorption of inactivated virus to an aluminium hydroxide adjuvant, can help mitigate global supply and the cost constraints of IPV. The objective of this trial was to demonstrate the non-inferiority of IPV-Al to standard IPV.
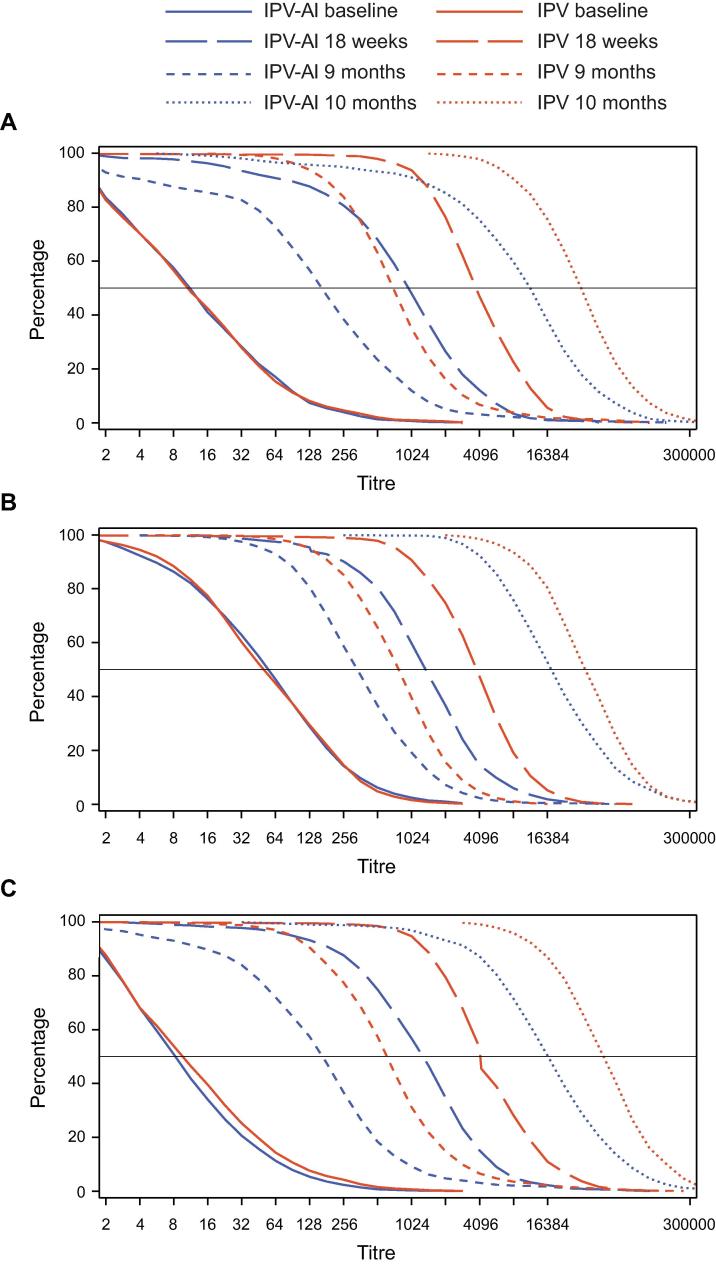
Methods: This phase 3, observer-blinded, randomised, controlled trial was conducted at 5 investigational sites in the Philippines. Infants not previously vaccinated with any polio vaccines were randomised to receive three IPV-Al (n = 502) or IPV vaccinations (n = 500) at 6, 10 and 14 weeks of age plus a booster vaccination at 9 months. The primary endpoint was type-specific seroconversion, defined as an antibody titre ≥4-fold higher than the estimated maternal antibody titre and a titre ≥8, one month after the primary vaccination series.
Results: Seroconversion rates following primary vaccination with IPV-Al (483 infants in the per-protocol analysis set) or IPV (478 infants) were: polio type 1, 97.1% versus 99.0%; type 2, 94.2% versus 99.0%; and type 3, 98.3% versus 99.6%. IPV-Al was non-inferior to IPV, as the lower 95% confidence limits of the treatment differences were above the predefined -10%-point limit: type 1, -1.85% (-3.85; -0.05); type 2, -4.75% (-7.28; -2.52); type 3, -1.24 (-2.84; 0.13). The booster effect (geometric mean titre (GMT) post-booster / GMT pre-booster) was: type 1, 63 versus 43; type 2, 54 versus 47; type 3, 112 versus 80. IPV-Al was well tolerated with a safety profile comparable to that of IPV. Serious adverse events were recorded for 29 infants (5.8%, 37 events) in the IPV-Al group compared to 28 (5.6%, 48 events) in the IPV group.
Conclusion: Non-inferiority of IPV-Al to IPV with respect to seroconversion was confirmed and a robust booster response was demonstrated. Both vaccines had a similar safety profile. ClinicalTrials.gov identifier: NCT03032419.
Keywords: Affordable IPV; Aluminium hydroxide adjuvant; Booster vaccination; Immunogenicity; Polio; Primary vaccination.
Copyright © 2019 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: [Birgit Thierry-Carstensen and Pernille Nyholm Tingskov are employees of Statens Serum Institut, a governmental non-profit research organization, and Charlotte Sørensen, Pernille Ingemann Nielsen and Mie Vestergaard Kusk are employees of AJ Vaccines A/S. Both Statens Serum Institut and AJ Vaccines A/S were involved in developing the vaccine at the time the trial was conducted. May Emmeline B. Montellano received research grants from Sanofi Pasteur and SK Chemicals. Ananda S. Bandyopadhyay is a full-time employee at the Bill & Melinda Gates Foundation].
Figures

References
-
- World Health Organization (WHO). Poliomyelitis.. 2019. Accessed 27Mar2019. https://www.who.int/en/news-room/fact-sheets/detail/poliomyelitis.
-
- World Health Organization (WHO). Polio eradication & endgame strategic plan 2013-2018. Geneva, Switzerland. WHO Press World Health Organization; 2013. Accessed 27Mar2019. http://polioeradicationorg/who-we-are/strategy/.
-
- Minor P. Vaccine-derived poliovirus (VDPV): Impact on poliomyelitis eradication. Vaccine. 2009;27:2649–2652. - PubMed
-
- Andreasen L.V., Hansen L.B., Andersen P., Agger E.M., Dietrich J. Aluminium hydroxide potentiates a protective Th1 biased immune response against polio virus that allows for dose sparing in mice and rats. Vaccine. 2015;33:1873–1879. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
