

An automated framework for localization, segmentation and super-resolution reconstruction of fetal brain MRI
- PMID: 31704293
- PMCID: PMC7103783
- DOI: 10.1016/j.neuroimage.2019.116324
An automated framework for localization, segmentation and super-resolution reconstruction of fetal brain MRI
Abstract
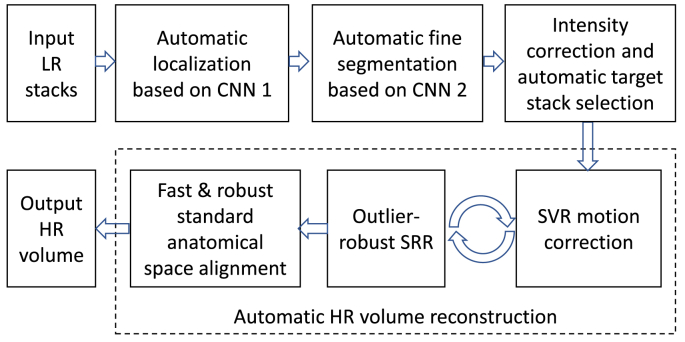
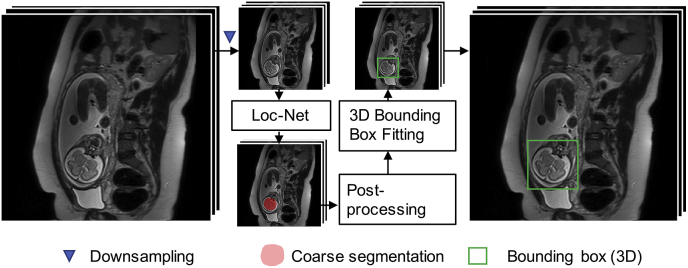
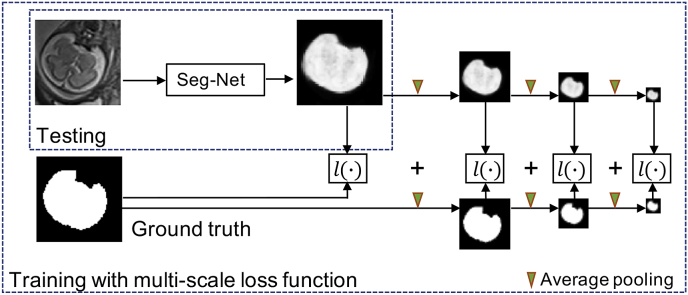
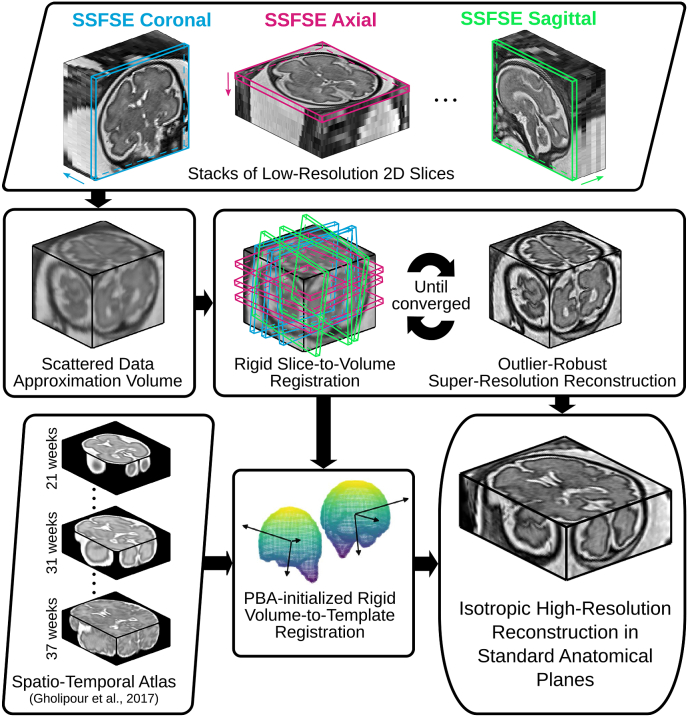
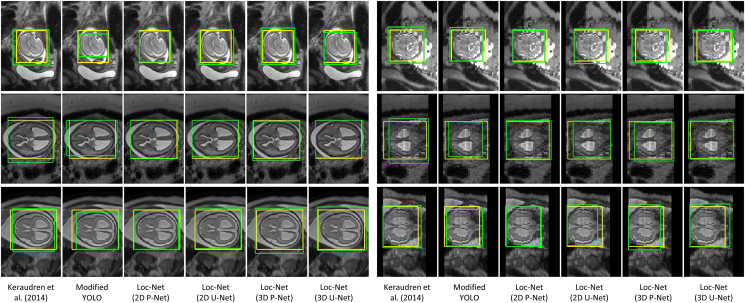
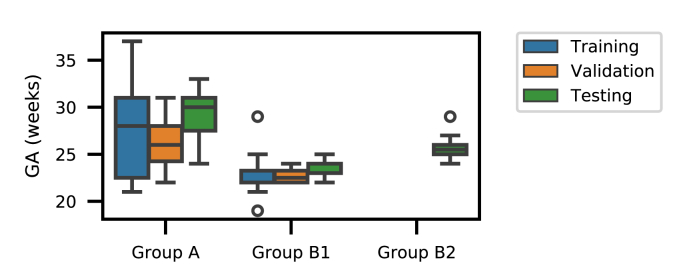
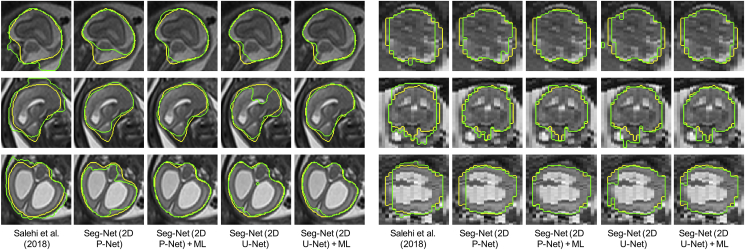
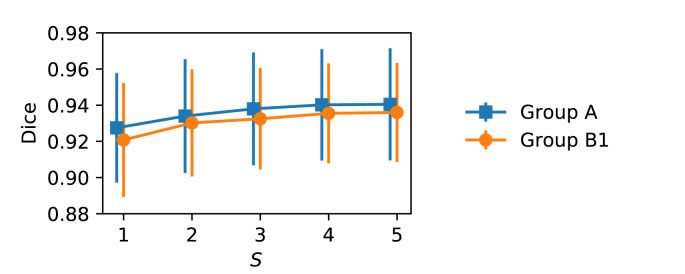
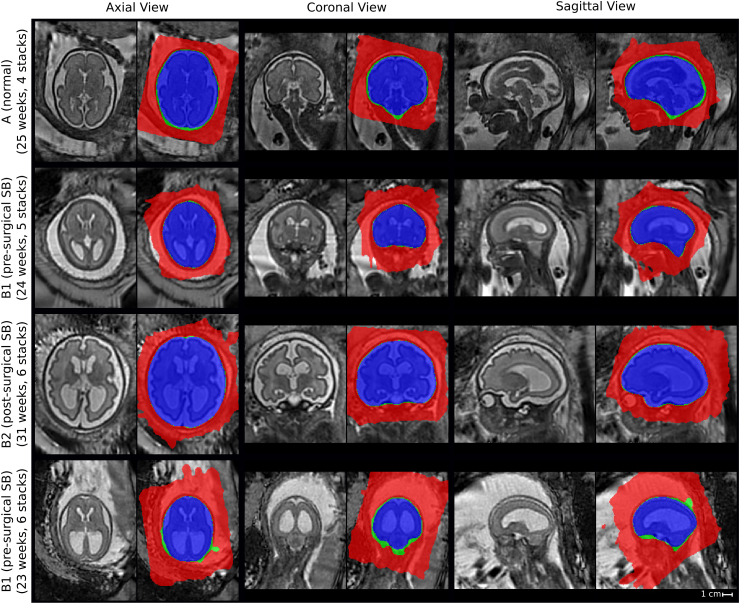
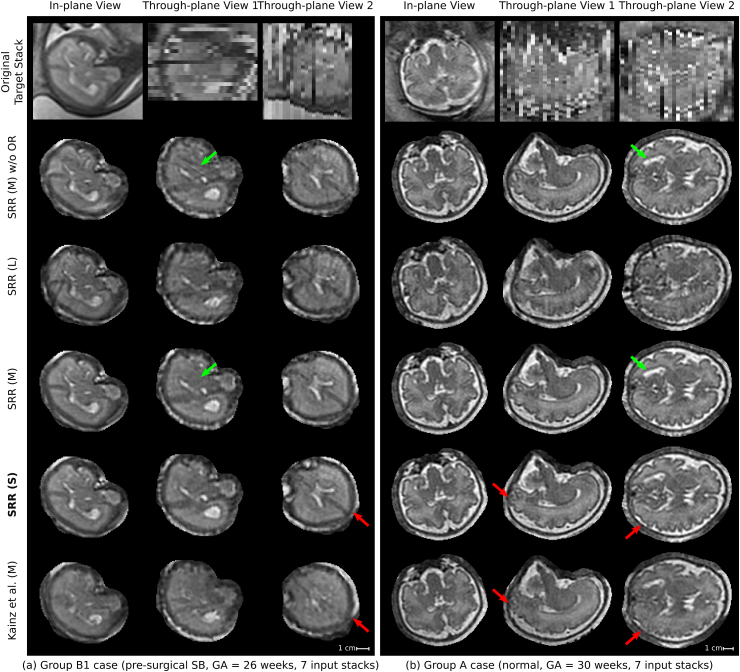
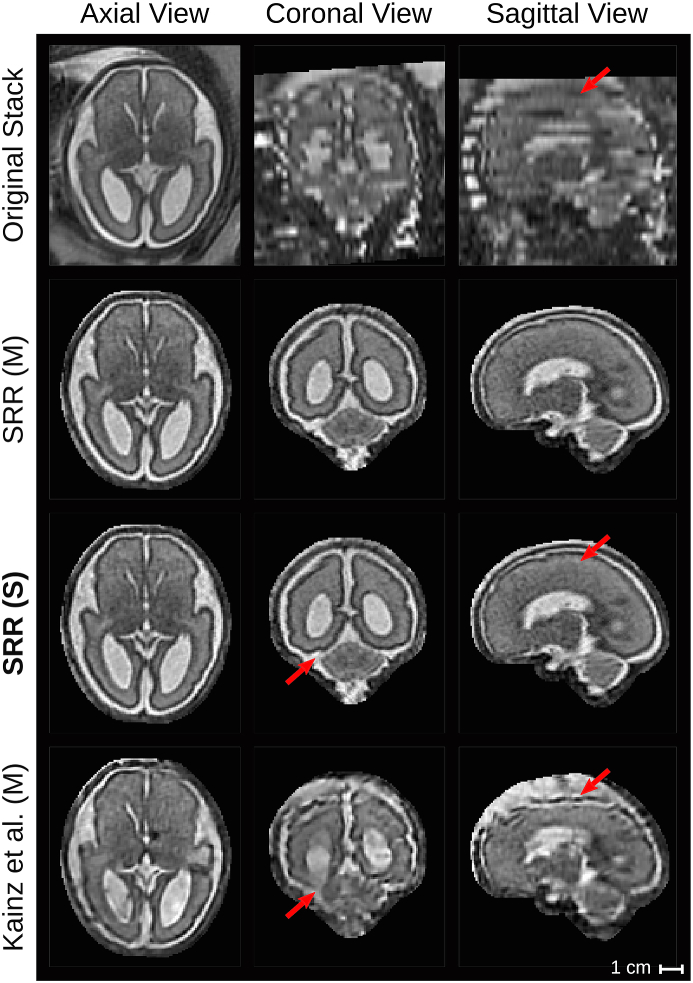
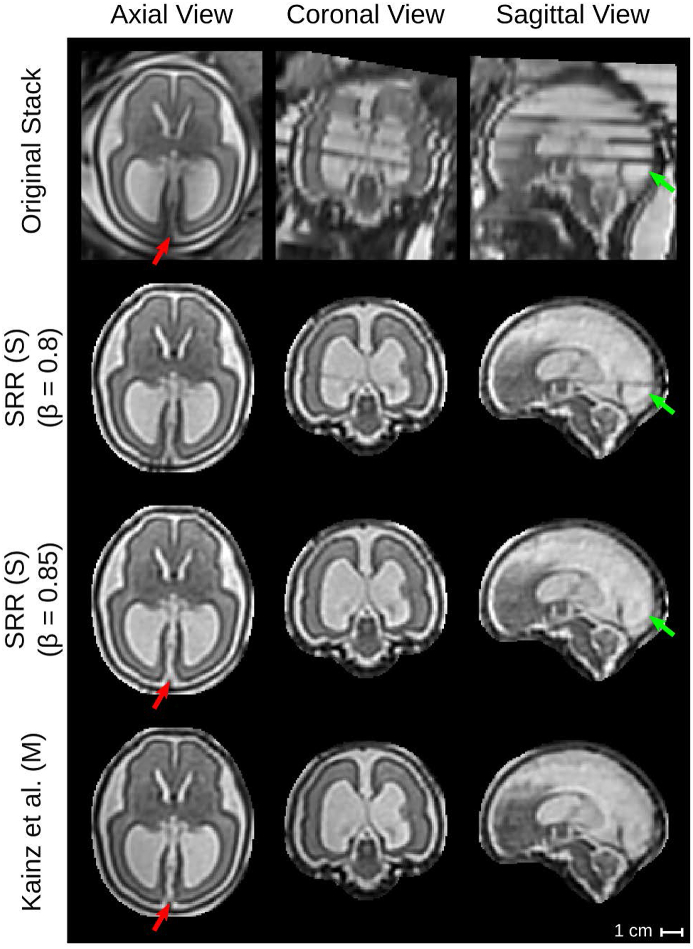
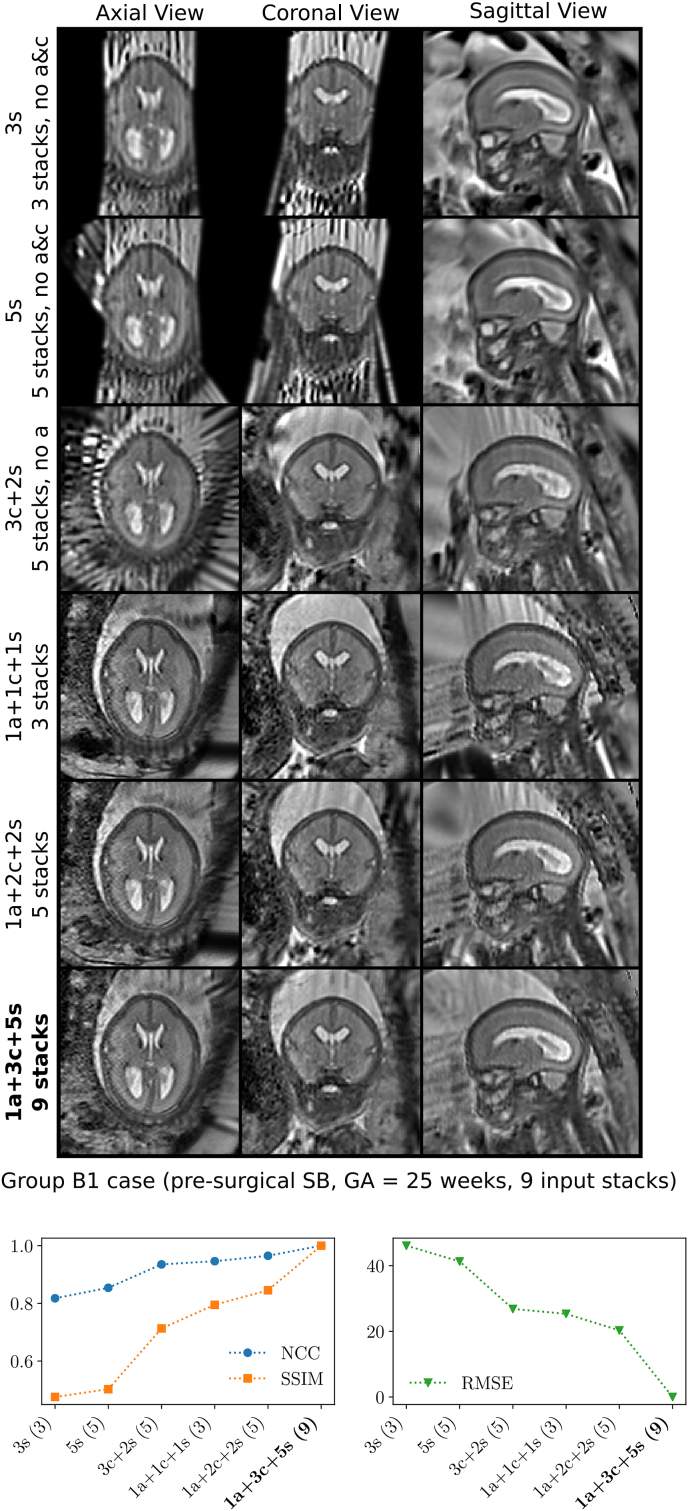
High-resolution volume reconstruction from multiple motion-corrupted stacks of 2D slices plays an increasing role for fetal brain Magnetic Resonance Imaging (MRI) studies. Currently existing reconstruction methods are time-consuming and often require user interactions to localize and extract the brain from several stacks of 2D slices. We propose a fully automatic framework for fetal brain reconstruction that consists of four stages: 1) fetal brain localization based on a coarse segmentation by a Convolutional Neural Network (CNN), 2) fine segmentation by another CNN trained with a multi-scale loss function, 3) novel, single-parameter outlier-robust super-resolution reconstruction, and 4) fast and automatic high-resolution visualization in standard anatomical space suitable for pathological brains. We validated our framework with images from fetuses with normal brains and with variable degrees of ventriculomegaly associated with open spina bifida, a congenital malformation affecting also the brain. Experiments show that each step of our proposed pipeline outperforms state-of-the-art methods in both segmentation and reconstruction comparisons including expert-reader quality assessments. The reconstruction results of our proposed method compare favorably with those obtained by manual, labor-intensive brain segmentation, which unlocks the potential use of automatic fetal brain reconstruction studies in clinical practice.
Keywords: Brain localization; Convolutional neural network; Deep learning; Fetal MRI; Segmentation; Super resolution.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
WL was employed by King's College London during most of the preparation of this work and was employed by the company Nvidia for the final editing and proofreading of the manuscript. SO is a founder and shareholder of BrainMiner Ltd, UK.
Figures


References
-
- Aertsen M., Verduyckt J., De Keyzer F., Vercauteren T., Van Calenbergh F., De Catte L., Dymarkowski S., Demaerel P., Deprest J. Reliability of MR imaging-based posterior fossa and brain stem measurements in open spinal dysraphism in the era of fetal surgery. Am. J. Neuroradiol. 2019;40:191–198. http://www.ajnr.org/lookup/doi/10.3174/ajnr.A5930 - DOI - PMC - PubMed
-
- Alansary A., Rajchl M., McDonagh S.G., Murgasova M., Damodaram M., Lloyd D.F.A., Davidson A., Rutherford M., Hajnal J.V., Rueckert D., Kainz B. PVR: patch-to-volume reconstruction for large area motion correction of fetal MRI. IEEE Trans. Med. Imaging. 2017;36:2031–2044. http://arxiv.org/abs/1611.07289 http://ieeexplore.ieee.org/document/8024032/ arXiv:1611.07289. - PMC - PubMed
-
- Anquez J., Angelini E.D., Bloch I. 2009 IEEE International Symposium on Biomedical Imaging: from Nano to Macro. IEEE; 2009. Automatic segmentation of head structures on fetal MRI; pp. 109–112.http://ieeexplore.ieee.org/lpdocs/epic03/wrapper.htm?arnumber=5192995
-
- Candès E.J., Li X., Ma Y., Wright J. Robust principal component analysis? J. Assoc. Comput. Mach. 2011;58:1–37. http://portal.acm.org/citation.cfm?doid=1970392.1970395
-
- Çiçek Ö., Abdulkadir A., Lienkamp S.S., Brox T., Ronneberger O. 3D U-net: learning dense volumetric segmentation from sparse annotation. In: Ourselin S., Joskowicz L., Sabuncu M.R., Unal G., Wells W., editors. Medical Image Computing and Computer-Assisted Intervention – MICCAI 2016. Springer International Publishing; Cham: 2016. pp. 424–432.http://link.springer.com/10.1007/978-3-319-46723-8{∖_}49 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
