

Absence of Islet Autoantibodies and Modestly Raised Glucose Values at Diabetes Diagnosis Should Lead to Testing for MODY: Lessons From a 5-Year Pediatric Swedish National Cohort Study
- PMID: 31704690
- PMCID: PMC6925576
- DOI: 10.2337/dc19-0747
Absence of Islet Autoantibodies and Modestly Raised Glucose Values at Diabetes Diagnosis Should Lead to Testing for MODY: Lessons From a 5-Year Pediatric Swedish National Cohort Study
Abstract
Objective: Identifying maturity-onset diabetes of the young (MODY) in pediatric populations close to diabetes diagnosis is difficult. Misdiagnosis and unnecessary insulin treatment are common. We aimed to identify the discriminatory clinical features at diabetes diagnosis of patients with glucokinase (GCK), hepatocyte nuclear factor-1A (HNF1A), and HNF4A MODY in the pediatric population.
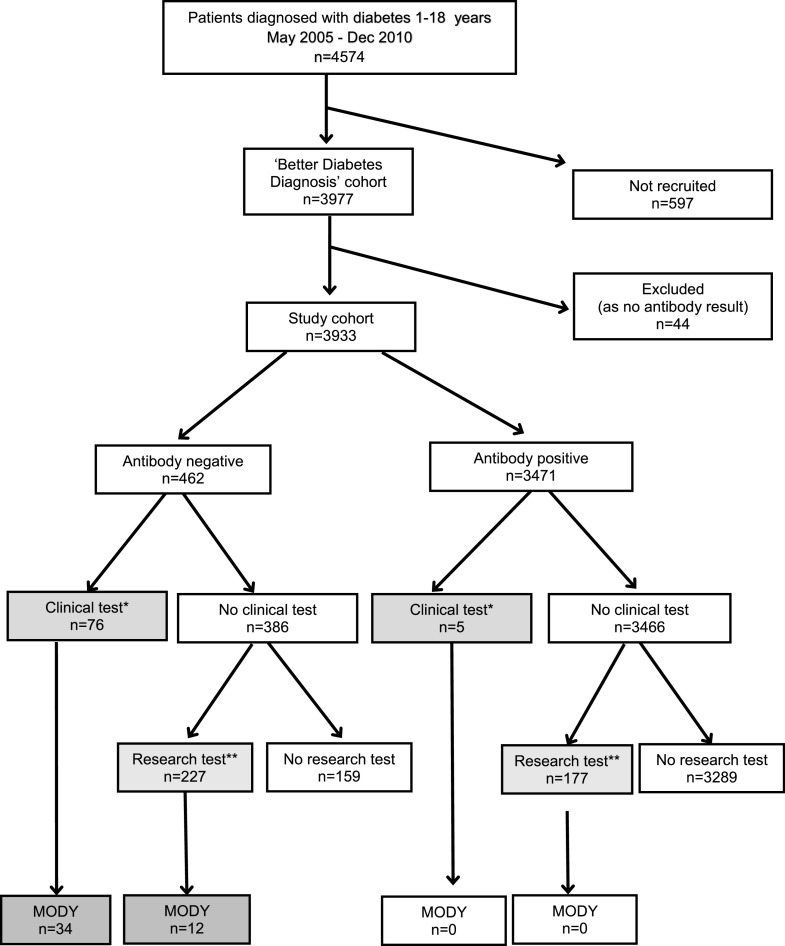
Research design and methods: Swedish patients (n = 3,933) aged 1-18 years, diagnosed with diabetes May 2005 to December 2010, were recruited from the national consecutive prospective cohort Better Diabetes Diagnosis. Clinical data, islet autoantibodies (GAD insulinoma antigen-2, zinc transporter 8, and insulin autoantibodies), HLA type, and C-peptide were collected at diagnosis. MODY was identified by sequencing GCK, HNF1A, and HNF4A, through either routine clinical or research testing.
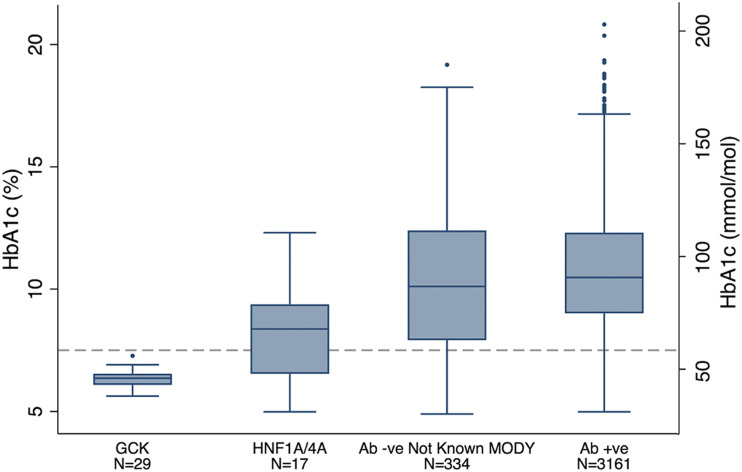
Results: The minimal prevalence of MODY was 1.2%. Discriminatory factors for MODY at diagnosis included four islet autoantibody negativity (100% vs. 11% not-known MODY; P = 2 × 10-44), HbA1c (7.0% vs. 10.7% [53 vs. 93 mmol/mol]; P = 1 × 10-20), plasma glucose (11.7 vs. 26.7 mmol/L; P = 3 × 10-19), parental diabetes (63% vs. 12%; P = 1 × 10-15), and diabetic ketoacidosis (0% vs. 15%; P = 0.001). Testing 303 autoantibody-negative patients identified 46 patients with MODY (detection rate 15%). Limiting testing to the 73 islet autoantibody-negative patients with HbA1c <7.5% (58 mmol/mol) at diagnosis identified 36 out of 46 (78%) patients with MODY (detection rate 49%). On follow-up, the 46 patients with MODY had excellent glycemic control, with an HbA1c of 6.4% (47 mmol/mol), with 42 out of 46 (91%) patients not on insulin treatment.
Conclusions: At diagnosis of pediatric diabetes, absence of all islet autoantibodies and modest hyperglycemia (HbA1c <7.5% [58 mmol/mol]) should result in testing for GCK, HNF1A, and HNF4A MODY. Testing all 12% patients negative for four islet autoantibodies is an effective strategy for not missing MODY but will result in a lower detection rate. Identifying MODY results in excellent long-term glycemic control without insulin.
© 2019 by the American Diabetes Association.
Figures
References
-
- Pihoker C, Gilliam LK, Ellard S, et al. .; SEARCH for Diabetes in Youth Study Group . Prevalence, characteristics and clinical diagnosis of maturity onset diabetes of the young due to mutations in HNF1A, HNF4A, and glucokinase: results from the SEARCH for Diabetes in Youth. J Clin Endocrinol Metab 2013;98:4055–4062 - PMC - PubMed
-
- Hattersley AT, Greeley SAW, Polak M, et al. . ISPAD Clinical Practice Consensus Guidelines 2018: the diagnosis and management of monogenic diabetes in children and adolescents. Pediatr Diabetes 2018;19(Suppl. 27):47–63 - PubMed
-
- Johansson BB, Irgens HU, Molnes J, et al. . Targeted next-generation sequencing reveals MODY in up to 6.5% of antibody-negative diabetes cases listed in the Norwegian Childhood Diabetes Registry. Diabetologia 2017;60:625–635 - PubMed
-
- Delvecchio M, Mozzillo E, Salzano G, et al. .; Diabetes Study Group of the Italian Society of Pediatric Endocrinology and Diabetes (ISPED) . Monogenic diabetes accounts for 6.3% of cases referred to 15 Italian pediatric diabetes centres during 2007 to 2012. J Clin Endocrinol Metab 2017;102:1826–1834 - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
