

Economic Evaluation of Extending Medicare Immunosuppressive Drug Coverage for Kidney Transplant Recipients in the Current Era
- PMID: 31704739
- PMCID: PMC6934999
- DOI: 10.1681/ASN.2019070646
Economic Evaluation of Extending Medicare Immunosuppressive Drug Coverage for Kidney Transplant Recipients in the Current Era
Abstract
Background: Kidney transplant recipients must take immunosuppressant drugs to prevent rejection and maintain transplant function. Medicare coverage of immunosuppressant drugs for kidney transplant recipients ceases 36 months after transplantation, potentially increasing the risk of transplant failure. A contemporary economic analysis of extending Medicare coverage for the duration of transplant survival using current costs of immunosuppressant medications in the era of generic equivalents may inform immunosuppressant drug policy.
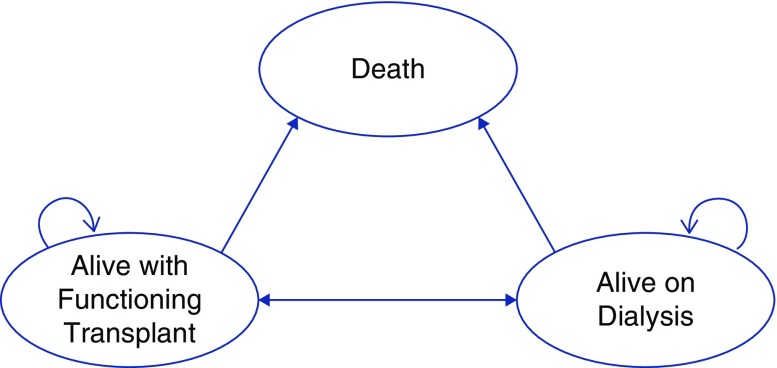
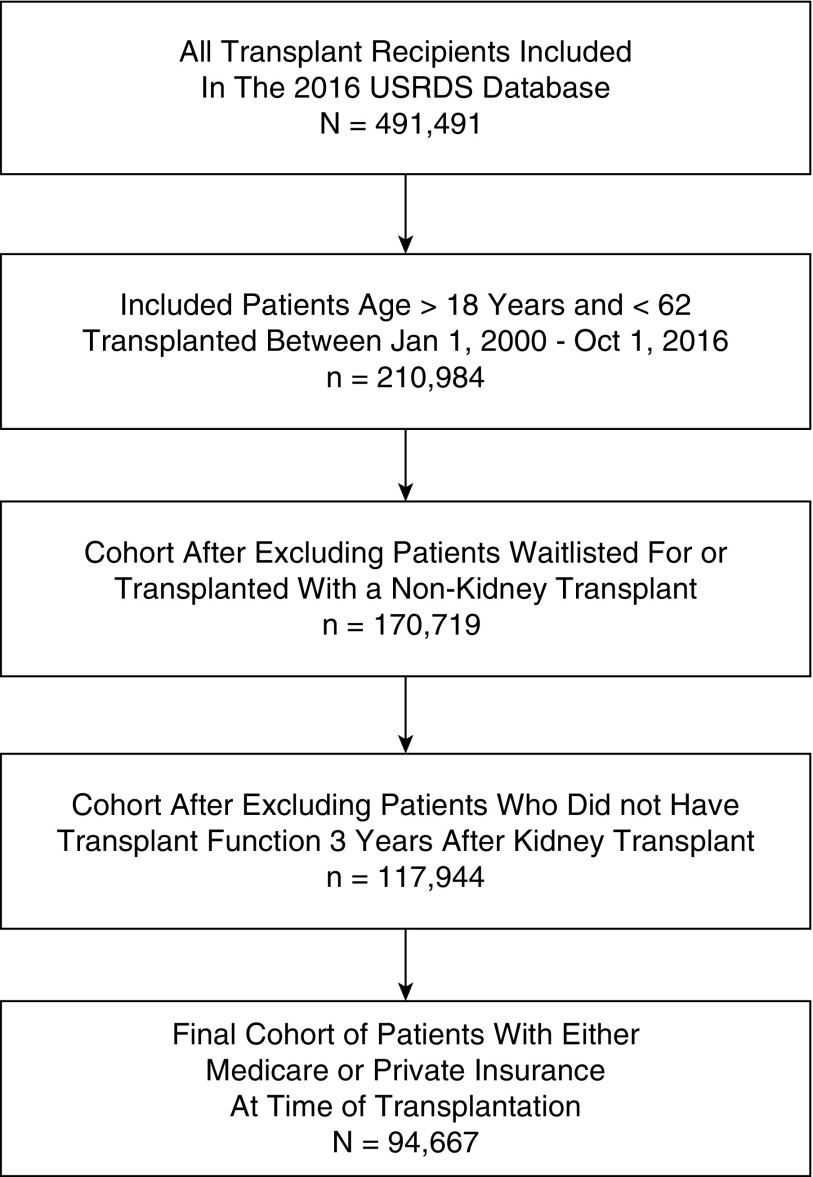
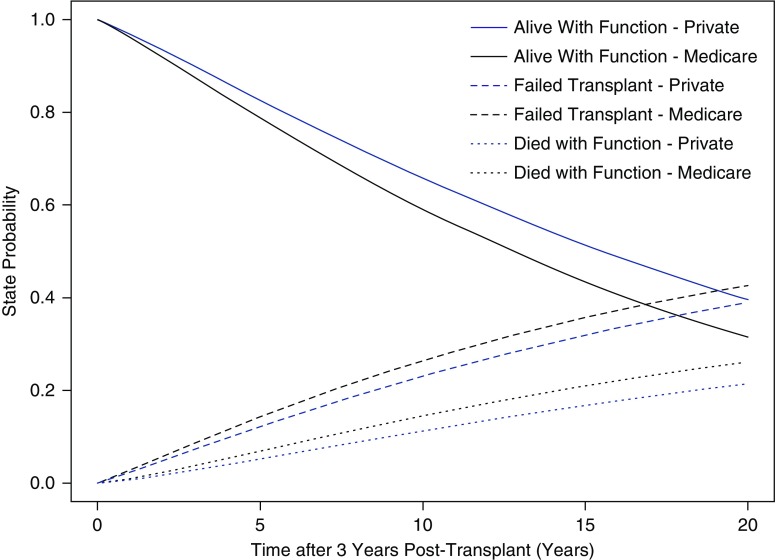
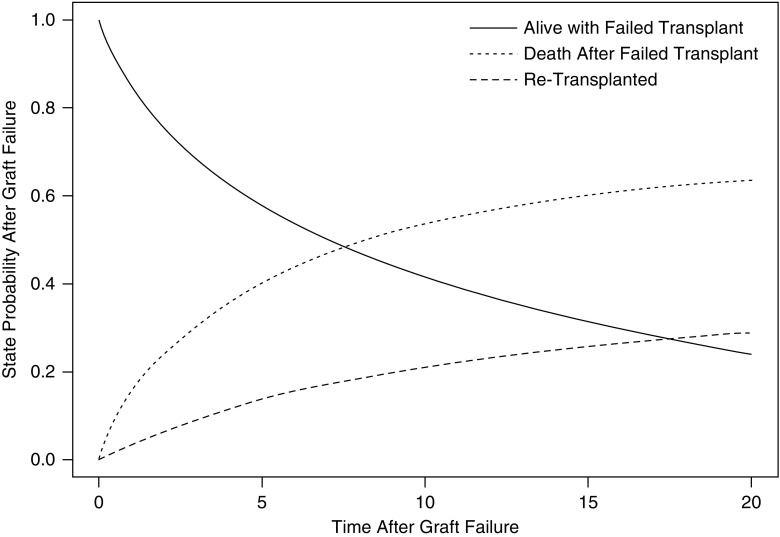
Methods: A Markov model was used to determine the incremental cost and effectiveness of extending Medicare coverage for immunosuppressive drugs over the duration of transplant survival, compared with the current policy of 36-month coverage, from the perspective of the Medicare payer. The expected improvement in transplant survival by extending immunosuppressive drug coverage was estimated from a cohort of privately insured transplant recipients who receive lifelong immunosuppressant drug coverage compared with a cohort of Medicare-insured transplant recipients, using multivariable survival analysis.
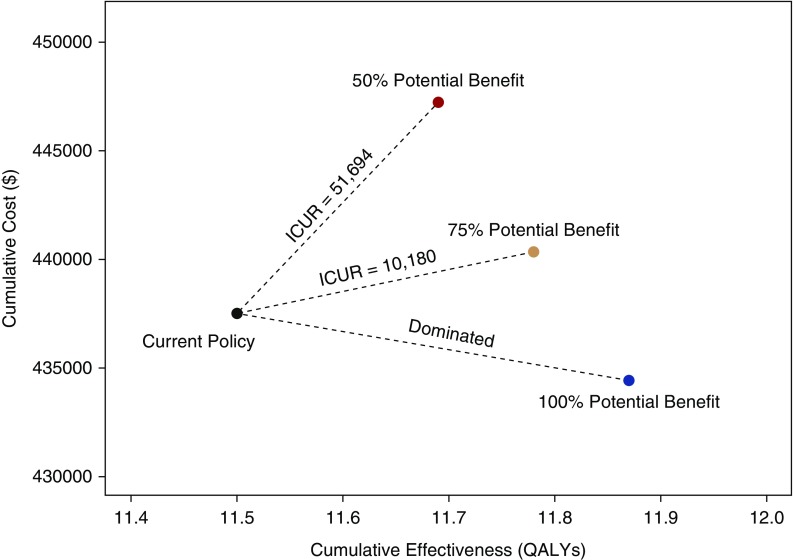
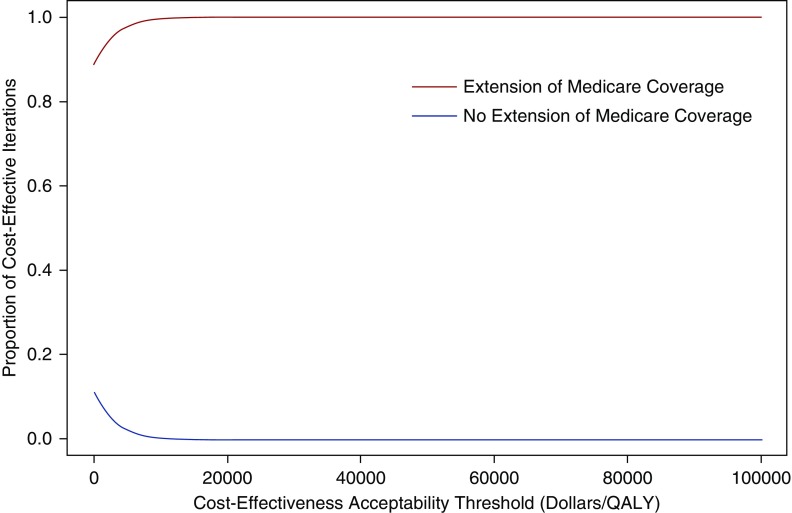
Results: Extension of immunosuppression Medicare coverage for kidney transplant recipients led to lower costs of -$3077 and 0.37 additional quality-adjusted life years (QALYs) per patient. When the improvement in transplant survival associated with extending immunosuppressant coverage was reduced to 50% of that observed in privately insured patients, the strategy of extending drug coverage had an incremental cost-utility ratio of $51,694 per QALY gained. In a threshold analysis, the extension of immunosuppression coverage was cost-effective at a willingness-to-pay threshold of $100,000, $50,000, and $0 per QALY if it results in a decrease in risk of transplant failure of 5.5%, 7.8%, and 13.3%, respectively.
Conclusions: Extending immunosuppressive drug coverage under Medicare from the current 36 months to the duration of transplant survival will result in better patient outcomes and cost-savings, and remains cost-effective if only a fraction of anticipated benefit is realized.
Keywords: Economic Analysis; Medicare; kidney transplantation; transplant outcomes.
Copyright © 2020 by the American Society of Nephrology.
Figures
References
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al.: Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 341: 1725–1730, 1999 - PubMed
-
- Laupacis A, Keown P, Pus N, Krueger H, Ferguson B, Wong C, et al.: A study of the quality of life and cost-utility of renal transplantation. Kidney Int 50: 235–242, 1996 - PubMed
-
- Axelrod DA, Schnitzler MA, Xiao H, Irish W, Tuttle-Newhall E, Chang SH, et al.: An economic assessment of contemporary kidney transplant practice. Am J Transplant 18: 1168–1176, 2018 - PubMed
-
- Tonelli M, Wiebe N, Knoll G, Bello A, Browne S, Jadhav D, et al.: Systematic review: Kidney transplantation compared with dialysis in clinically relevant outcomes. Am J Transplant 11: 2093–2109, 2011 - PubMed
-
- United States Renal Data System : 2018 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2018
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
