

Appropriate coronary revascularization can be accomplished if myocardial perfusion is quantified by positron emission tomography prior to treatment decision
- PMID: 31705424
- PMCID: PMC8421314
- DOI: 10.1007/s12350-019-01938-y
Appropriate coronary revascularization can be accomplished if myocardial perfusion is quantified by positron emission tomography prior to treatment decision
Abstract
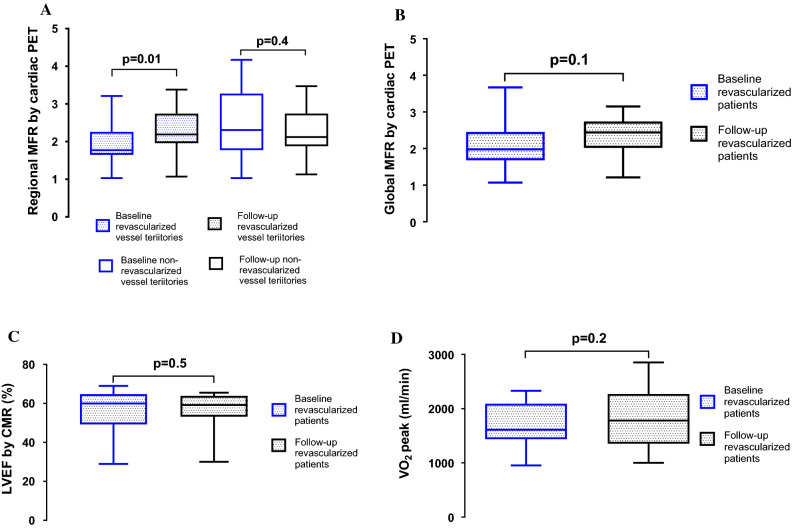
Background: Many patients undergo percutaneous coronary intervention (PCI) without the use of non-invasive stress testing prior to treatment. The aim of this study was to determine the potential added value of guiding revascularization by quantitative assessment of myocardial perfusion prior to intervention.
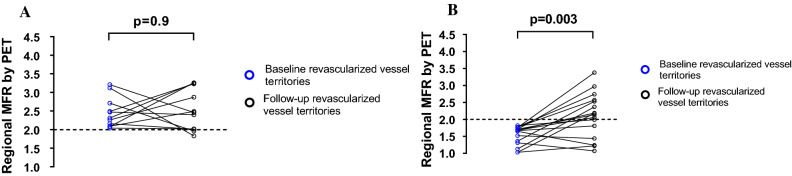
Methods and results: Thirty-three patients (10 females) with suspected or established CAD who had been referred for a clinical coronary angiography (CA) with possibility for PCI were included. Adenosine stress and rest 13N-NH3 PET, cardiac magnetic resonance (CMR), and cardiopulmonary exercise test were performed 4 ± 3 weeks before and 5 ± 1 months after CA. The angiographer was blinded to the PET and CMR results. Myocardial flow reserve (MFR) < 2.0 by PET was considered abnormal. A PCI was performed in 19/33 patients. In 41% (11/27) of the revascularized vessel territories, a normal regional MFR was found prior to the PCI and no improvement in MFR was found at follow-up (P = 0.9). However, vessel territories with regional MFR < 2.0 at baseline improved significantly after PCI (P = 0.003). Of the 14 patients not undergoing PCI, four had MFR < 2.0 in one or more coronary territories.
Conclusion: Assessment of quantitative myocardial perfusion prior to revascularization could lead to more appropriate use of CA when managing patients with stable CAD.
Keywords: Coronary artery disease; coronary angiography; revascularization; stress imaging.
© 2019. The Author(s).
Figures

References
-
- Task Force M, Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34:2949–3003. doi: 10.1093/eurheartj/eht296. - DOI - PubMed
-
- Shaw LJ, Berman DS, Maron DJ, Mancini GB, Hayes SW, Hartigan PM, et al. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: Results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation. 2008;117:1283–1291. doi: 10.1161/CIRCULATIONAHA.107.743963. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
