

Effects of a swallowing and oral care intervention for patients following endotracheal extubation: a pre- and post-intervention study
- PMID: 31706360
- PMCID: PMC6842457
- DOI: 10.1186/s13054-019-2623-2
Effects of a swallowing and oral care intervention for patients following endotracheal extubation: a pre- and post-intervention study
Abstract
Background: For patients who survive a critical illness and have their oral endotracheal tube removed, dysphagia is highly prevalent, and without intervention, it may persist far beyond hospital discharge. This pre- and post-intervention study with historical controls tested the effects of a swallowing and oral care (SOC) intervention on patients' time to resume oral intake and salivary flow following endotracheal extubation.
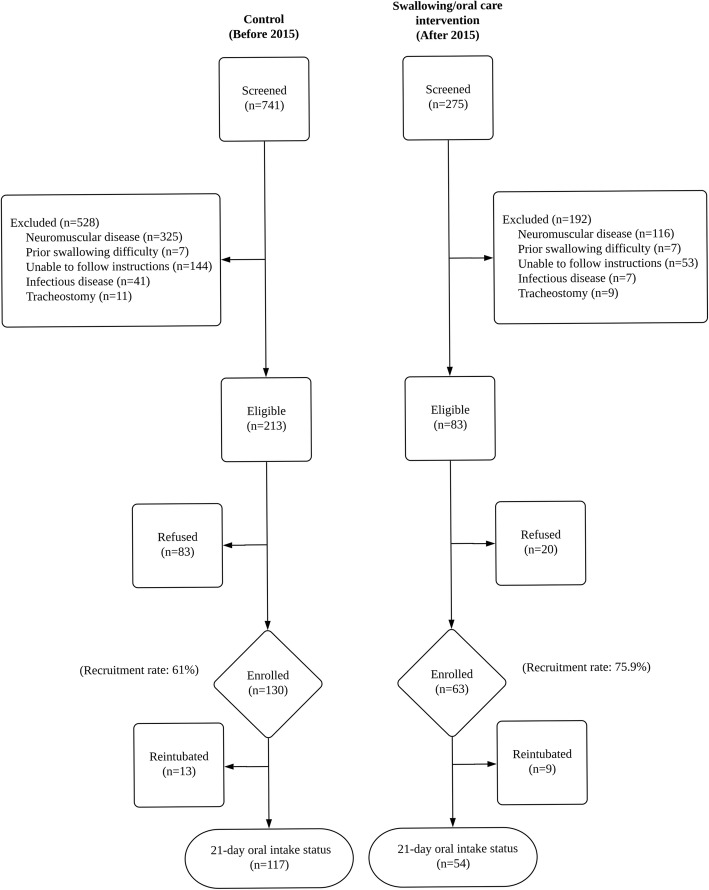
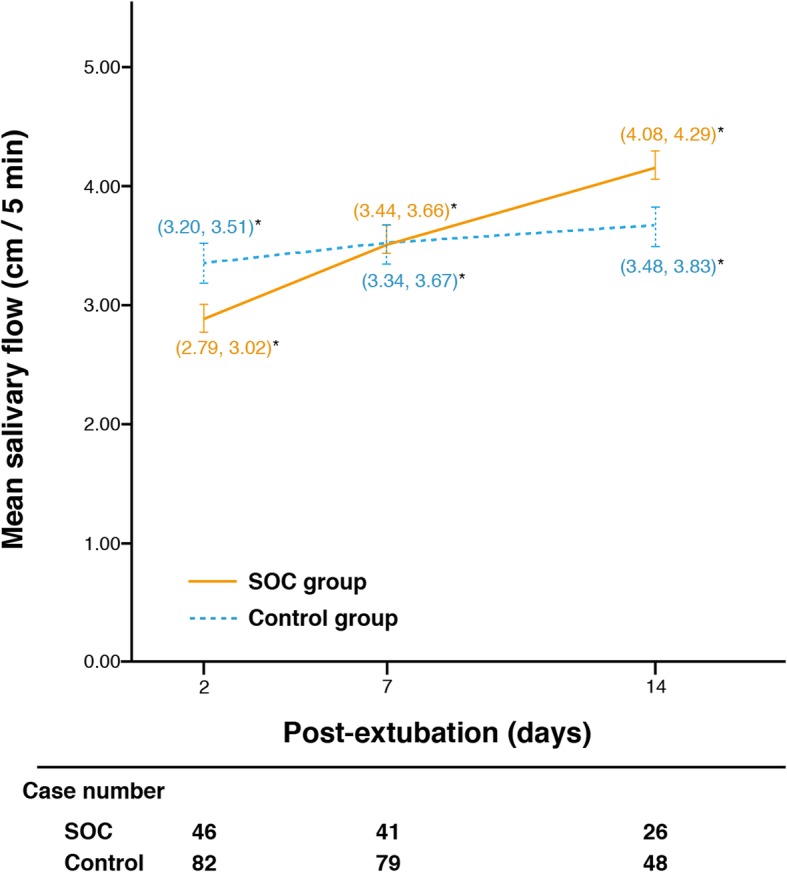
Methods: The sample comprised intensive care unit patients (≥ 50 years) successfully extubated after ≥ 48 h endotracheal intubation. Participants who received usual care (controls, n = 117) were recruited before 2015, and those who received usual care plus the intervention (n = 54) were enrolled after 2015. After extubation, all participants were assessed by a blinded nurse for daily intake status (21 days) and whole-mouth unstimulated salivary flow (2, 7, 14 days). The intervention group received the nurse-administered SOC intervention, comprising toothbrushing/salivary gland massage, oral motor exercise, and safe-swallowing education daily for 14 days or until hospital discharge.
Results: The intervention group received 8.3 ± 4.2 days of SOC intervention, taking 15.4 min daily with no reported adverse event (coughing, wet voice, or decreased oxygen saturation) during and immediately after intervention. Participants who received the intervention were significantly more likely than controls to resume total oral intake after extubation (aHR 1.77, 95% CI 1.08-2.91). Stratified by age group, older participants (≥ 65 years) in the SOC group were 2.47-fold more likely than their younger counterparts to resume total oral intake (aHR 2.47, 95% CI 1.31-4.67). The SOC group also had significantly higher salivary flows 14 days following extubation (β = 0.67, 95% CI 0.29-1.06).
Conclusions: The nurse-administered SOC is safe and effective, with greater odds of patients' resuming total oral intake and increased salivary flows 14 days following endotracheal extubation. Age matters with SOC; it more effectively helped participants ≥ 65 years old resume total oral intake postextubation.
Trial registration: NCT02334774, registered on January 08, 2015.
Keywords: Critical illness; Dysphagia; Endotracheal intubation; Oral intake; Salivation; Swallowing.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Effects of a swallowing and oral-care program on resuming oral feeding and reducing pneumonia in patients following endotracheal extubation: a randomized, open-label, controlled trial.Crit Care. 2023 Jul 12;27(1):283. doi: 10.1186/s13054-023-04568-6. Crit Care. 2023. PMID: 37438759 Free PMC article. Clinical Trial.
-
Effectiveness of Swallowing and Oral Care Interventions on Oral Intake and Salivary Flow of Patients Following Endotracheal Extubation at a Tertiary Care Center: A Randomized Controlled Trial.J Caring Sci. 2023 Nov 12;12(4):213-220. doi: 10.34172/jcs.2023.33005. eCollection 2023 Dec. J Caring Sci. 2023. PMID: 38250001 Free PMC article.
-
Predicting feeding-tube dependence in patients following endotracheal extubation: a two-item swallowing screen.BMC Pulm Med. 2021 Dec 6;21(1):403. doi: 10.1186/s12890-021-01771-5. BMC Pulm Med. 2021. PMID: 34872549 Free PMC article.
-
A Decision Guide for Assessing the Recently Extubated Patient's Readiness for Safe Oral Intake.Crit Care Nurse. 2023 Feb 1;43(1):42-51. doi: 10.4037/ccn2023722. Crit Care Nurse. 2023. PMID: 36720280 Review.
-
Prevention of unplanned endotracheal extubation in intensive care unit: An overview of systematic reviews.Nurs Open. 2023 Feb;10(2):392-403. doi: 10.1002/nop2.1317. Epub 2022 Aug 15. Nurs Open. 2023. PMID: 35971250 Free PMC article. Review.
Cited by
-
Effects of a swallowing and oral-care program on resuming oral feeding and reducing pneumonia in patients following endotracheal extubation: a randomized, open-label, controlled trial.Crit Care. 2023 Jul 12;27(1):283. doi: 10.1186/s13054-023-04568-6. Crit Care. 2023. PMID: 37438759 Free PMC article. Clinical Trial.
-
[Postextubation dysphagia : Challenges regarding interdisciplinary collaboration in intensive care units].Med Klin Intensivmed Notfmed. 2025 Jul 22. doi: 10.1007/s00063-025-01304-6. Online ahead of print. Med Klin Intensivmed Notfmed. 2025. PMID: 40694071 Review. German.
-
Effectiveness of Swallowing and Oral Care Interventions on Oral Intake and Salivary Flow of Patients Following Endotracheal Extubation at a Tertiary Care Center: A Randomized Controlled Trial.J Caring Sci. 2023 Nov 12;12(4):213-220. doi: 10.34172/jcs.2023.33005. eCollection 2023 Dec. J Caring Sci. 2023. PMID: 38250001 Free PMC article.
-
Interventions for Postextubation Dysphagia in Critically Ill Patients: A Systematic Review and Meta-analysis.Dysphagia. 2024 Dec;39(6):1013-1024. doi: 10.1007/s00455-024-10695-1. Epub 2024 Apr 1. Dysphagia. 2024. PMID: 38558176
-
[Postextubation dysphagia in intensive care patients : Current findings and clinical recommendations].Anaesthesiologie. 2022 Jul;71(7):546-555. doi: 10.1007/s00101-022-01092-0. Epub 2022 Feb 15. Anaesthesiologie. 2022. PMID: 35166868 Review. German.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
