

Healthcare trajectories before and after critical illness: population-based insight on diverse patients clusters
- PMID: 31707487
- PMCID: PMC6842359
- DOI: 10.1186/s13613-019-0599-3
Healthcare trajectories before and after critical illness: population-based insight on diverse patients clusters
Abstract
Background: The post intensive care syndrome (PICS) gathers various disabilities, associated with a substantial healthcare use. However, patients' comorbidities and active medical conditions prior to intensive care unit (ICU) admission may partly drive healthcare use after ICU discharge. To better understand retative contribution of critical illness and PICS-compared to pre-existing comorbidities-as potential determinant of post-critical illness healthcare use, we conducted a population-based evaluation of patients' healthcare use trajectories.
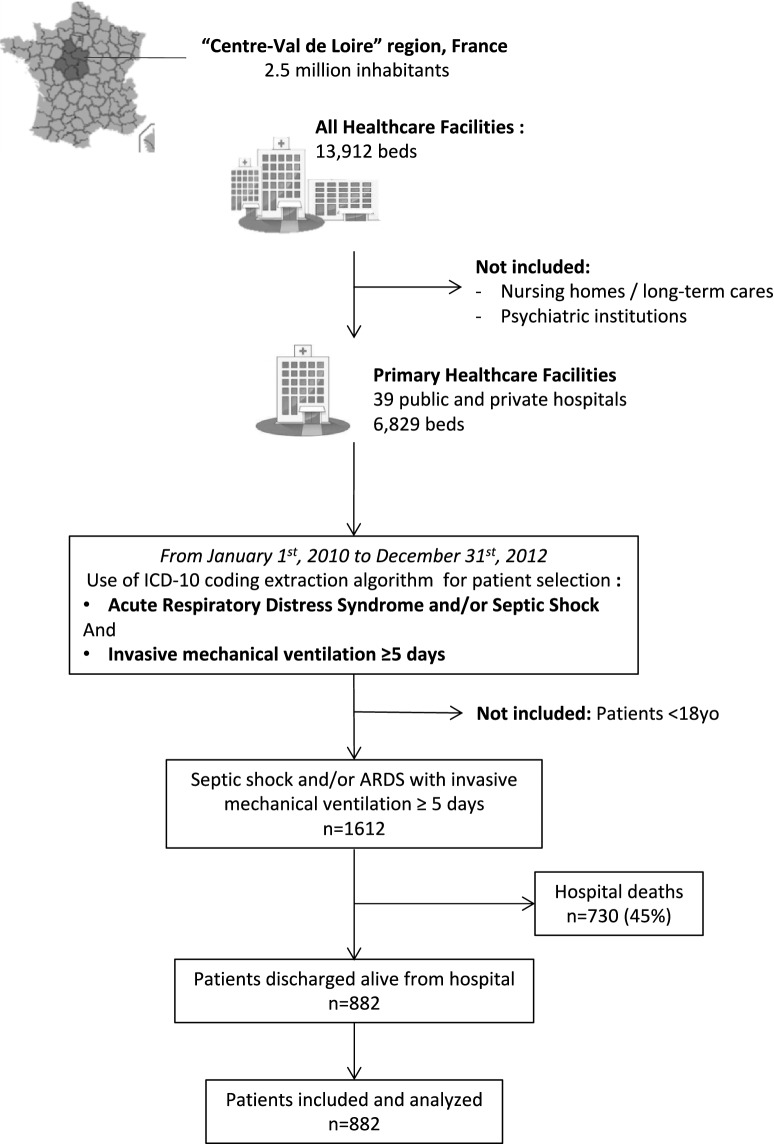
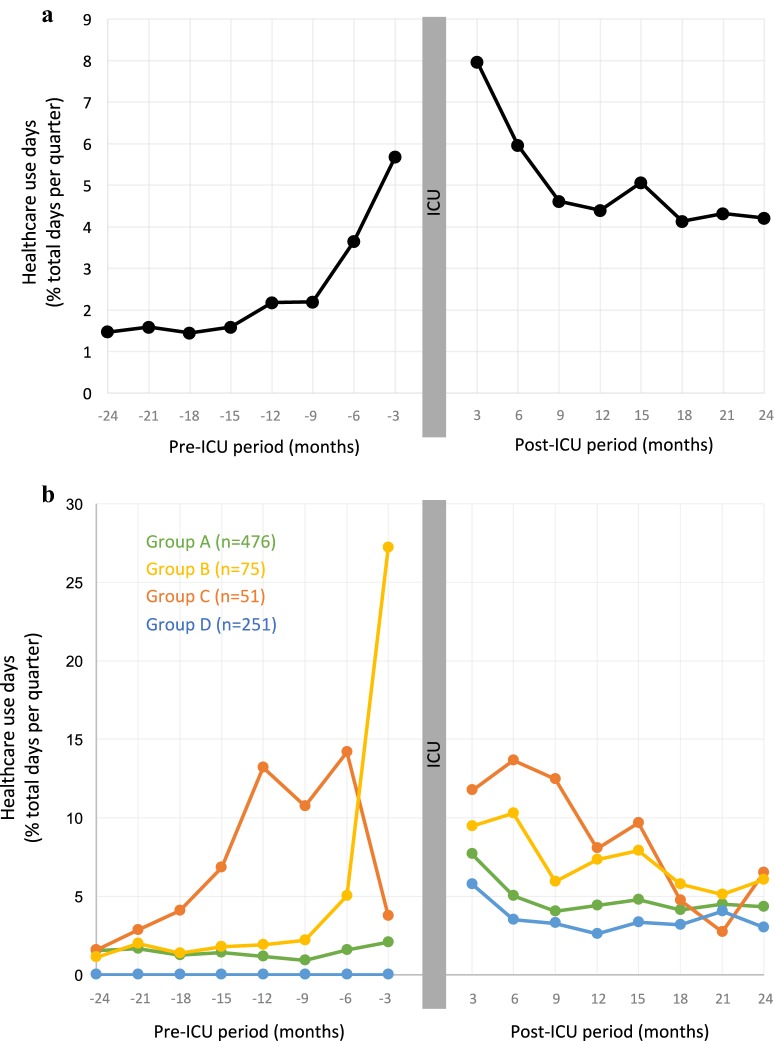
Results: Using discharge databases in a 2.5-million-people region in France, we retrieved, over 3 years, all adult patients admitted in ICU for septic shock or acute respiratory distress syndrome (ARDS), intubated at least 5 days and discharged alive from hospital: 882 patients were included. Median duration of mechanical ventilation was 11 days (interquartile ranges [IQR] 8;20), mean SAPS2 was 49, and median hospital length of stay was 42 days (IQR 29;64). Healthcare use (days spent in healthcare facilities) was analyzed 2 years before and 2 years after ICU admission. Prior to ICU admission, we observed, at the scale of the whole study population, a progressive increase in healthcare use. Healthcare trajectories were then explored at individual level, and patients were assembled according to their individual pre-ICU healthcare use trajectory by clusterization with the K-Means method. Interestingly, this revealed diverse trajectories, identifying patients with elevated and increasing healthcare use (n = 126), and two main groups with low (n = 476) or no (n = 251) pre-ICU healthcare use. In ICU, however, SAPS2, duration of mechanical ventilation and length of stay were not different across the groups. Analysis of post-ICU healthcare trajectories for each group revealed that patients with low or no pre-ICU healthcare (which represented 83% of the population) switched to a persistent and elevated healthcare use during the 2 years post-ICU.
Conclusion: For 83% of ARDS/septic shock survivors, critical illness appears to have a pivotal role in healthcare trajectories, with a switch from a low and stable healthcare use prior to ICU to a sustained higher healthcare recourse 2 years after ICU discharge. This underpins the hypothesis of long-term critical illness and PICS-related quantifiable consequences in healthcare use, measurable at a population level.
Keywords: Acute respiratory distress syndrome; Healthcare trajectories; Long-term outcome; Post-intensive care syndrome; Septic shock.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Needham DM, Davidson J, Cohen H, Hopkins RO, Weinert C, Wunsch H, et al. Improving long-term outcomes after discharge from intensive care unit. Crit Care Med. 2012;40(2):502–509. - PubMed
-
- Elliott D, Davidson JE, Harvey MA, Bemis-Dougherty A, Hopkins RO, Iwashyna TJ, et al. Exploring the scope of post-intensive care syndrome therapy and care: engagement of non-critical care providers and survivors in a second stakeholders meeting. Crit Care Med. 2014;42(12):2518–2526. - PubMed
-
- Harvey MA, Davidson JE. Postintensive care syndrome. Crit Care Med. 2016;44(2):381–385. - PubMed
LinkOut - more resources
Full Text Sources
