

Dobutamine Stress Echocardiography Ischemia as a Predictor of the Placebo-Controlled Efficacy of Percutaneous Coronary Intervention in Stable Coronary Artery Disease: The Stress Echocardiography-Stratified Analysis of ORBITA
- PMID: 31707827
- PMCID: PMC6903430
- DOI: 10.1161/CIRCULATIONAHA.119.042918
Dobutamine Stress Echocardiography Ischemia as a Predictor of the Placebo-Controlled Efficacy of Percutaneous Coronary Intervention in Stable Coronary Artery Disease: The Stress Echocardiography-Stratified Analysis of ORBITA
Abstract
Background: Dobutamine stress echocardiography is widely used to test for ischemia in patients with stable coronary artery disease. In this analysis, we studied the ability of the prerandomization stress echocardiography score to predict the placebo-controlled efficacy of percutaneous coronary intervention (PCI) within the ORBITA trial (Objective Randomised Blinded Investigation With Optimal Medical Therapy of Angioplasty in Stable Angina).
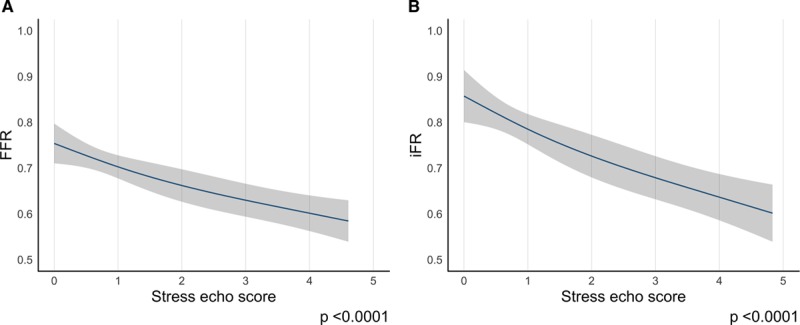
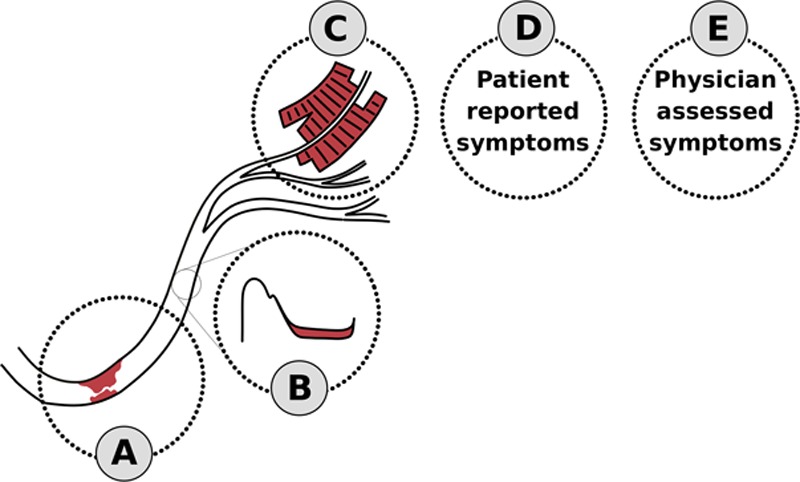
Methods: One hundred eighty-three patients underwent dobutamine stress echocardiography before randomization. The stress echocardiography score is broadly the number of segments abnormal at peak stress, with akinetic segments counting double and dyskinetic segments counting triple. The ability of prerandomization stress echocardiography to predict the placebo-controlled effect of PCI on response variables was tested by using regression modeling.
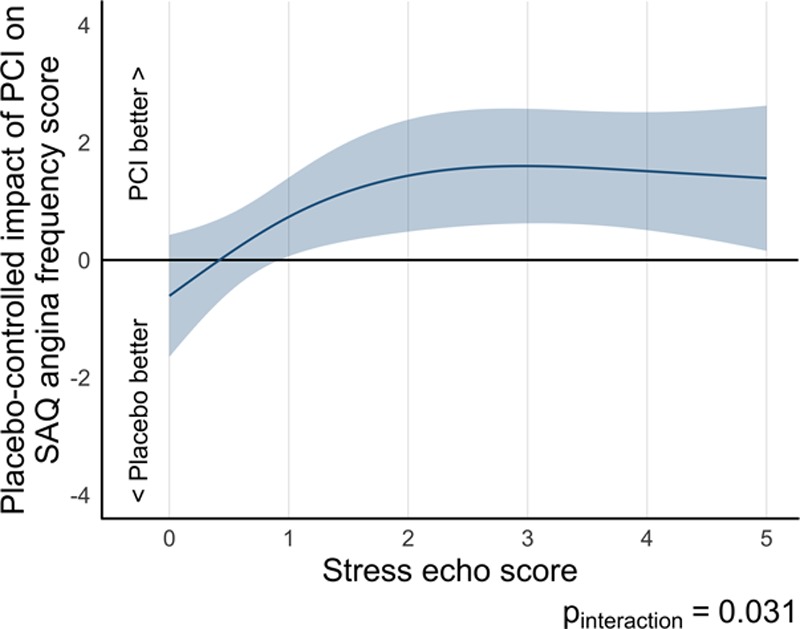
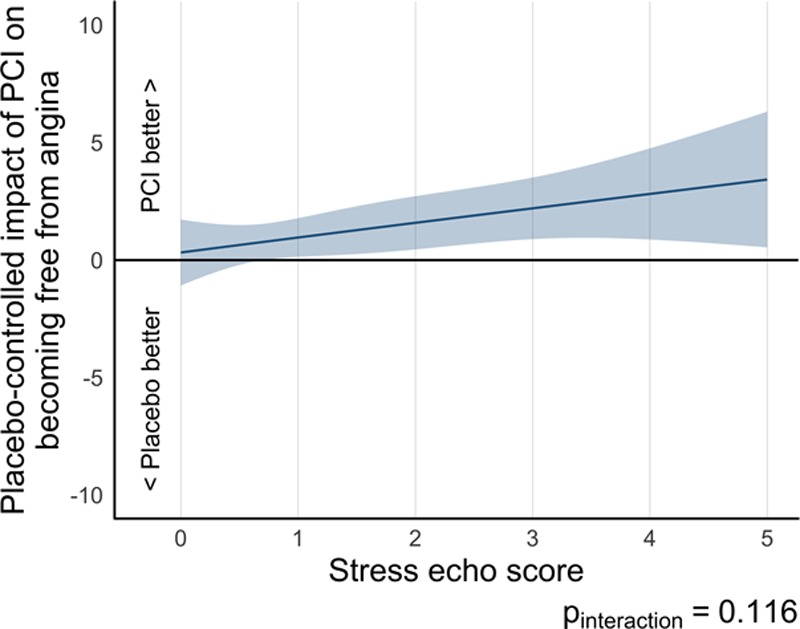
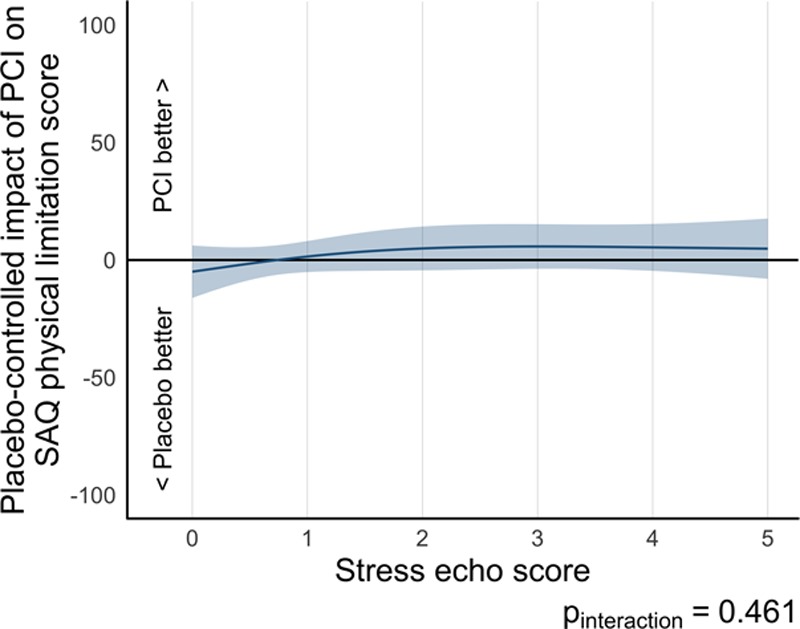
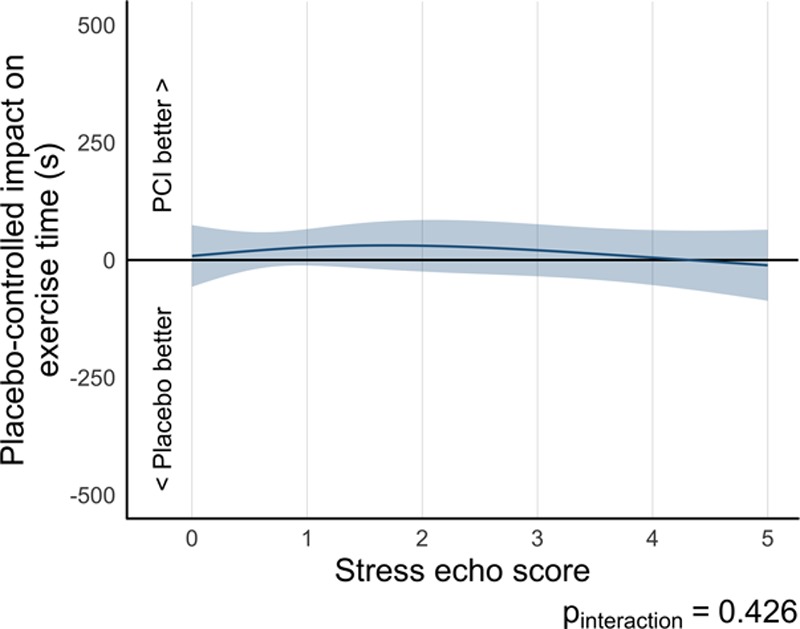
Results: At prerandomization, the stress echocardiography score was 1.56±1.77 in the PCI arm (n=98) and 1.61±1.73 in the placebo arm (n=85). There was a detectable interaction between prerandomization stress echocardiography score and the effect of PCI on angina frequency score with a larger placebo-controlled effect in patients with the highest stress echocardiography score (Pinteraction=0.031). With our sample size, we were unable to detect an interaction between stress echocardiography score and any other patient-reported response variables: freedom from angina (Pinteraction=0.116), physical limitation (Pinteraction=0.461), quality of life (Pinteraction=0.689), EuroQOL 5 quality-of-life score (Pinteraction=0.789), or between stress echocardiography score and physician-assessed Canadian Cardiovascular Society angina class (Pinteraction=0.693), and treadmill exercise time (Pinteraction=0.426).
Conclusions: The degree of ischemia assessed by dobutamine stress echocardiography predicts the placebo-controlled efficacy of PCI on patient-reported angina frequency. The greater the downstream stress echocardiography abnormality caused by a stenosis, the greater the reduction in symptoms from PCI.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT02062593.
Keywords: angina, stable; coronary artery disease; echocardiography, stress; percutaneous coronary intervention.
Figures
Comment in
-
A Leap Forward for Ischemia-Guided Revascularization: Stress Echocardiography Predicts Angina Benefit With Percutaneous Coronary Intervention.Circulation. 2019 Dec 10;140(24):1981-1983. doi: 10.1161/CIRCULATIONAHA.119.044026. Epub 2019 Nov 11. Circulation. 2019. PMID: 31707830 No abstract available.
References
-
- Al-Lamee R, Thompson D, Dehbi HM, Sen S, Tang K, Davies J, Keeble T, Mielewczik M, Kaprielian R, Malik IS, et al. ORBITA Investigators. Percutaneous coronary intervention in stable angina (ORBITA): a double-blind, randomised controlled trial. Lancet. 2018;391:31–40. doi: 10.1016/S0140-6736(17)32714-9. - PubMed
-
- Weintraub WS, Spertus JA, Kolm P, Maron DJ, Zhang Z, Jurkovitz C, Zhang W, Hartigan PM, Lewis C, Veledar E, et al. COURAGE Trial Research Group. Effect of PCI on quality of life in patients with stable coronary disease. N Engl J Med. 2008;359:677–687. doi: 10.1056/NEJMoa072771. - PubMed
-
- Frye RL, August P, Brooks MM, Hardison RM, Kelsey SF, MacGregor JM, Orchard TJ, Chaitman BR, Genuth SM, Goldberg SH, et al. BARI 2D Study Group. A randomized trial of therapies for type 2 diabetes and coronary artery disease. N Engl J Med. 2009;360:2503–2515. doi: 10.1056/NEJMoa0805796. - PMC - PubMed
-
- De Bruyne B, Fearon WF, Pijls NH, Barbato E, Tonino P, Piroth Z, Jagic N, Mobius-Winckler S, Rioufol G, Witt N, et al. FAME 2 Trial Investigators. Fractional flow reserve-guided PCI for stable coronary artery disease. N Engl J Med. 2014;371:1208–1217. doi: 10.1056/NEJMoa1408758. - PubMed
-
- Windecker S, Stortecky S, Stefanini GG, da Costa BR, Rutjes AW, Di Nisio M, Silletta MG, Maione A, Alfonso F, Clemmensen PM, et al. Revascularisation versus medical treatment in patients with stable coronary artery disease: network meta-analysis. BMJ. 2014;348:g3859. doi: 10.1136/bmj.g3859. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
