

Coronary Microvascular Dysfunction Is Associated With Myocardial Ischemia and Abnormal Coronary Perfusion During Exercise
- PMID: 31707835
- PMCID: PMC6882540
- DOI: 10.1161/CIRCULATIONAHA.119.041595
Coronary Microvascular Dysfunction Is Associated With Myocardial Ischemia and Abnormal Coronary Perfusion During Exercise
Abstract
Background: Coronary microvascular dysfunction (MVD) is defined by impaired flow augmentation in response to a pharmacological vasodilator in the presence of nonobstructive coronary artery disease. It is unknown whether diminished coronary vasodilator response correlates with abnormal exercise physiology or inducible myocardial ischemia.
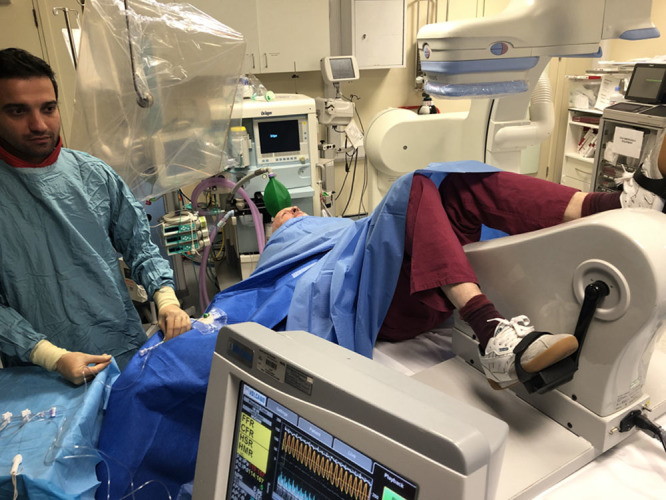
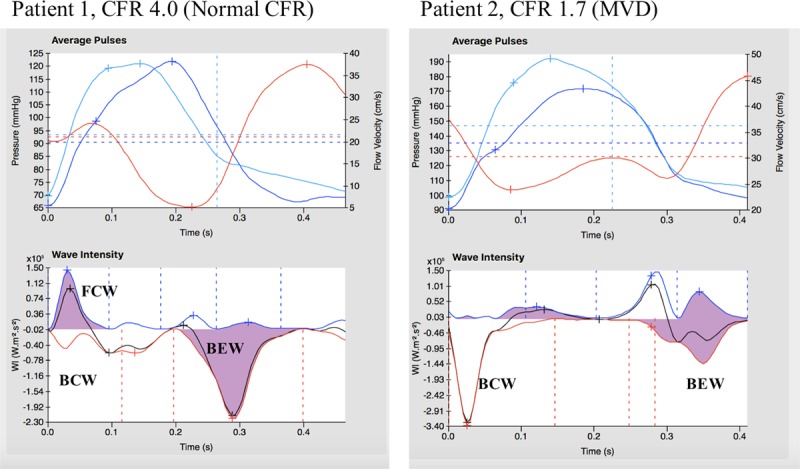
Methods: Patients with angina and nonobstructive coronary artery disease had simultaneous coronary pressure and flow velocity measured using a dual sensor-tipped guidewire during rest, supine bicycle exercise, and adenosine-mediated hyperemia. Microvascular resistance (MR) was calculated as coronary pressure divided by flow velocity. Wave intensity analysis quantified the proportion of accelerating wave energy (perfusion efficiency). Global myocardial blood flow and subendocardial:subepicardial perfusion ratio were quantified using 3-Tesla cardiac magnetic resonance imaging during hyperemia and rest; inducible ischemia was defined as hyperemic subendocardial:subepicardial perfusion ratio <1.0. Patients were classified as having MVD if coronary flow reserve <2.5 and controls if coronary flow reserve ≥2.5, with researchers blinded to the classification.
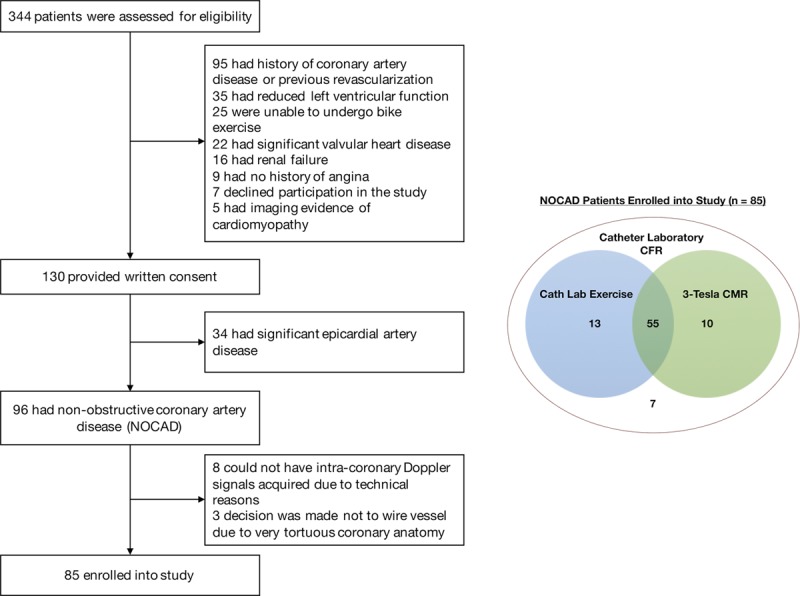
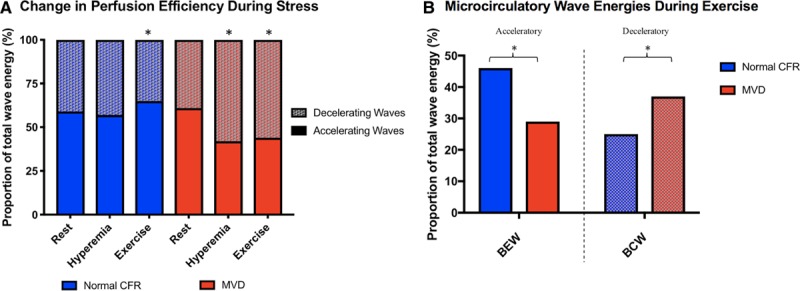
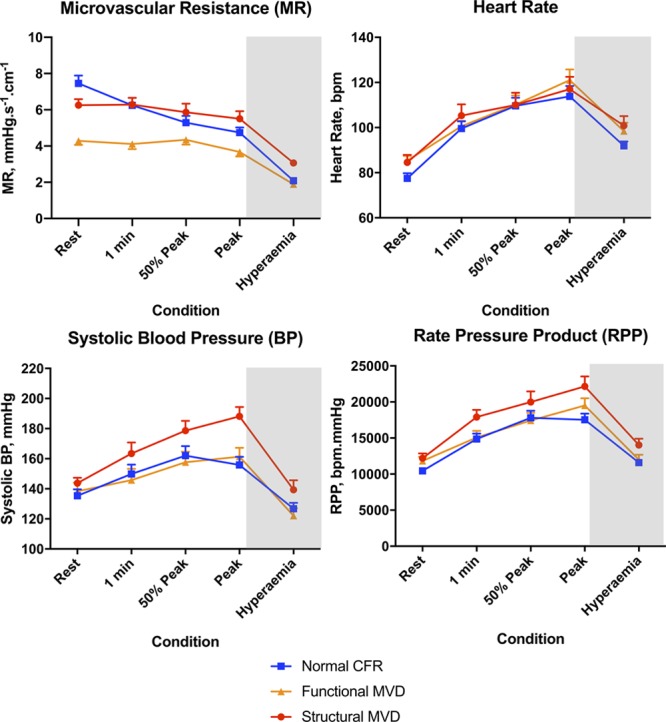
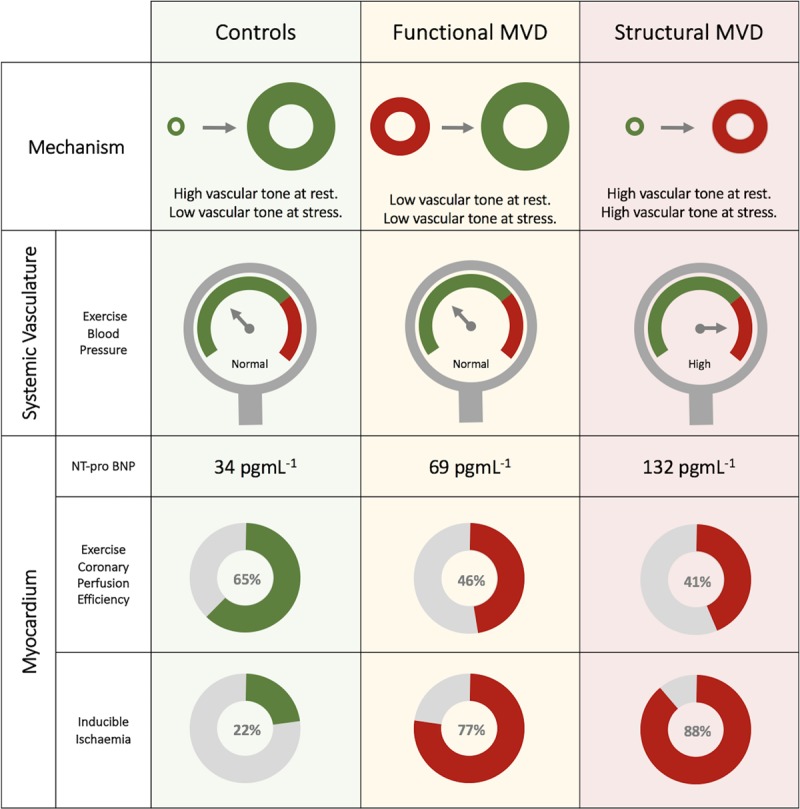
Results: Eighty-five patients were enrolled (78% female, 57±10 years), 45 (53%) were classified as having MVD. Of the MVD group, 82% had inducible ischemia compared with 22% of controls (P<0.001); global myocardial perfusion reserve was 2.01±0.41 and 2.68±0.49 (P<0.001). In controls, coronary perfusion efficiency improved from rest to exercise and was unchanged during hyperemia (59±11% vs 65±14% vs 57±18%; P=0.02 and P=0.14). In contrast, perfusion efficiency decreased during both forms of stress in MVD (61±12 vs 44±10 vs 42±11%; both P<0.001). Among patients with a coronary flow reserve <2.5, 62% had functional MVD, with normal minimal MR (hyperemic MR<2.5 mmHg/cm/s), and 38% had structural MVD with elevated hyperemic MR. Resting MR was lower in those with functional MVD (4.2±1.0 mmHg/cm/s) than in those with structural MVD (6.9±1.7 mmHg/cm/s) or controls (7.3±2.2 mmHg/cm/s; both P<0.001). During exercise, the structural group had a higher systolic blood pressure (188±25 mmHg) than did those with functional MVD (161±27 mmHg; P=0.004) and controls (156±30 mmHg; P<0.001). Functional and structural MVD had similar stress myocardial perfusion and exercise perfusion efficiency values.
Conclusion: In patients with angina and nonobstructive coronary artery disease, diminished coronary flow reserve characterizes a cohort with inducible ischemia and a maladaptive physiological response to exercise. We have identified 2 endotypes of MVD with distinctive systemic vascular responses to exercise; whether endotypes have a different prognosis or require different treatments merits further investigation.
Keywords: coronary artery disease; exercise; microvascular angina; perfusion imaging.
Figures
Comment in
-
The Shifting Sands of Coronary Microvascular Dysfunction.Circulation. 2019 Nov 26;140(22):1817-1819. doi: 10.1161/CIRCULATIONAHA.119.043952. Epub 2019 Nov 11. Circulation. 2019. PMID: 31707789 No abstract available.
References
-
- Likoff W, Segal BL, Kasparian H. Paradox of normal selective coronary arteriograms in patients considered to have unmistakable coronary heart disease. N Engl J Med. 1967;276:1063–1066. doi: 10.1056/NEJM196705112761904. - PubMed
-
- Bugiardini R, Bairey Merz CN. Angina with “normal” coronary arteries: a changing philosophy. JAMA. 2005;293:477–484. doi: 10.1001/jama.293.4.477. - PubMed
-
- Cannon RO, 3rd, Epstein SE. “Microvascular angina” as a cause of chest pain with angiographically normal coronary arteries. Am J Cardiol. 1988;61:1338–1343. doi: 10.1016/0002-9149(88)91180-0. - PubMed
-
- Pepine CJ, Anderson RD, Sharaf BL, Reis SE, Smith KM, Handberg EM, Johnson BD, Sopko G, Bairey Merz CN. Coronary microvascular reactivity to adenosine predicts adverse outcome in women evaluated for suspected ischemia results from the National Heart, Lung and Blood Institute WISE (Women’s Ischemia Syndrome Evaluation) study. J Am Coll Cardiol. 2010;55:2825–2832. doi: 10.1016/j.jacc.2010.01.054. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
