

Defining 'actionable' high- costhealth care use: results using the Canadian Institute for Health Information population grouping methodology
- PMID: 31707981
- PMCID: PMC6842471
- DOI: 10.1186/s12939-019-1074-3
Defining 'actionable' high- costhealth care use: results using the Canadian Institute for Health Information population grouping methodology
Abstract
Background: A small proportion of the population consumes the majority of health care resources. High-cost health care users are a heterogeneous group. We aim to segment a provincial population into relevant homogenous sub-groups to provide actionable information on risk factors associated with high-cost health care use within sub-populations.
Methods: The Canadian Institute for Health Information (CIHI) Population Grouping methodology was used to define mutually exclusive and clinically relevant health profile sub-groups. High-cost users (> = 90th percentile of health care spending) were defined within each sub-group. Univariate analyses explored demographic, socio-economic status, health status and health care utilization variables associated with high-cost use. Multivariable logistic regression models were constructed for the costliest health profile groups.
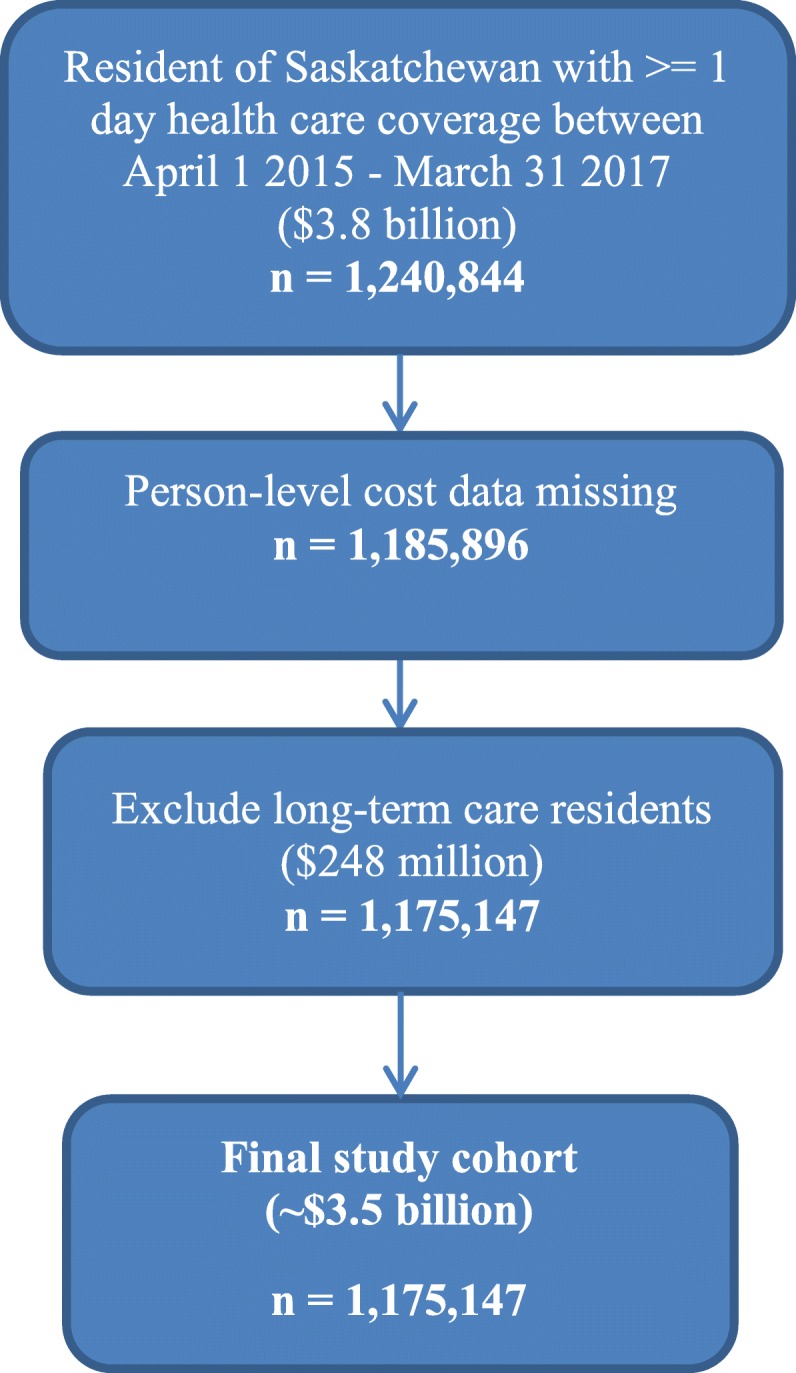
Results: From 2015 to 2017, 1,175,147 individuals were identified for study. High-cost users consumed 41% of total health care resources. Average annual health care spending for individuals not high-cost were $642; high-cost users were $16,316. The costliest health profile groups were 'long-term care', 'palliative', 'major acute', 'major chronic', 'major cancer', 'major newborn', 'major mental health' and 'moderate chronic'. Both 'major acute' and 'major cancer' health profile groups were largely explained by measures of health care utilization and multi-morbidity. In the remaining costliest health profile groups modelled, 'major chronic', 'moderate chronic', 'major newborn' and 'other mental health', a measure of socio-economic status, low neighbourhood income, was statistically significantly associated with high-cost use.
Interpretation: Model results point to specific, actionable information within clinically meaningful subgroups to reduce high-cost health care use. Health equity, specifically low socio-economic status, was statistically significantly associated with high-cost use in the majority of health profile sub-groups. Population segmentation methods, and more specifically, the CIHI Population Grouping Methodology, provide specificity to high-cost health care use; informing interventions aimed at reducing health care costs and improving population health.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Akaike H. Information theory and an extension of the maximum likelihood principle. In: Petrov BN, Csáki F, editors. 2nd International Symposium on Information Theory, Tsahkadsor, Armenia. Budapest: Akadémiai Kiadó; 1973;267–81.
-
- Anderson Maureen, Revie Crawford W., Quail Jacqueline M., Wodchis Walter, de Oliveira Claire, Osman Meriç, Baetz Marilyn, McClure J., Stryhn Henrik, Buckeridge David, Neudorf Cordell. The effect of socio-demographic factors on mental health and addiction high-cost use: a retrospective, population-based study in Saskatchewan. Canadian Journal of Public Health. 2018;109(5-6):810–820. doi: 10.17269/s41997-018-0101-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
