

Kidney damage and associated risk factors in rural and urban sub-Saharan Africa (AWI-Gen): a cross-sectional population study
- PMID: 31708144
- PMCID: PMC7033368
- DOI: 10.1016/S2214-109X(19)30443-7
Kidney damage and associated risk factors in rural and urban sub-Saharan Africa (AWI-Gen): a cross-sectional population study
Abstract
Background: Rapid epidemiological health transitions occurring in vulnerable populations in Africa that have an existing burden of infectious and non-communicable diseases predict an increased risk and consequent prevalence of kidney disease. However, few studies have characterised the true burden of kidney damage and associated risk factors in Africans. We investigated the prevalence of markers for kidney damage and known risk factors in rural and urban settings in sub-Saharan Africa.
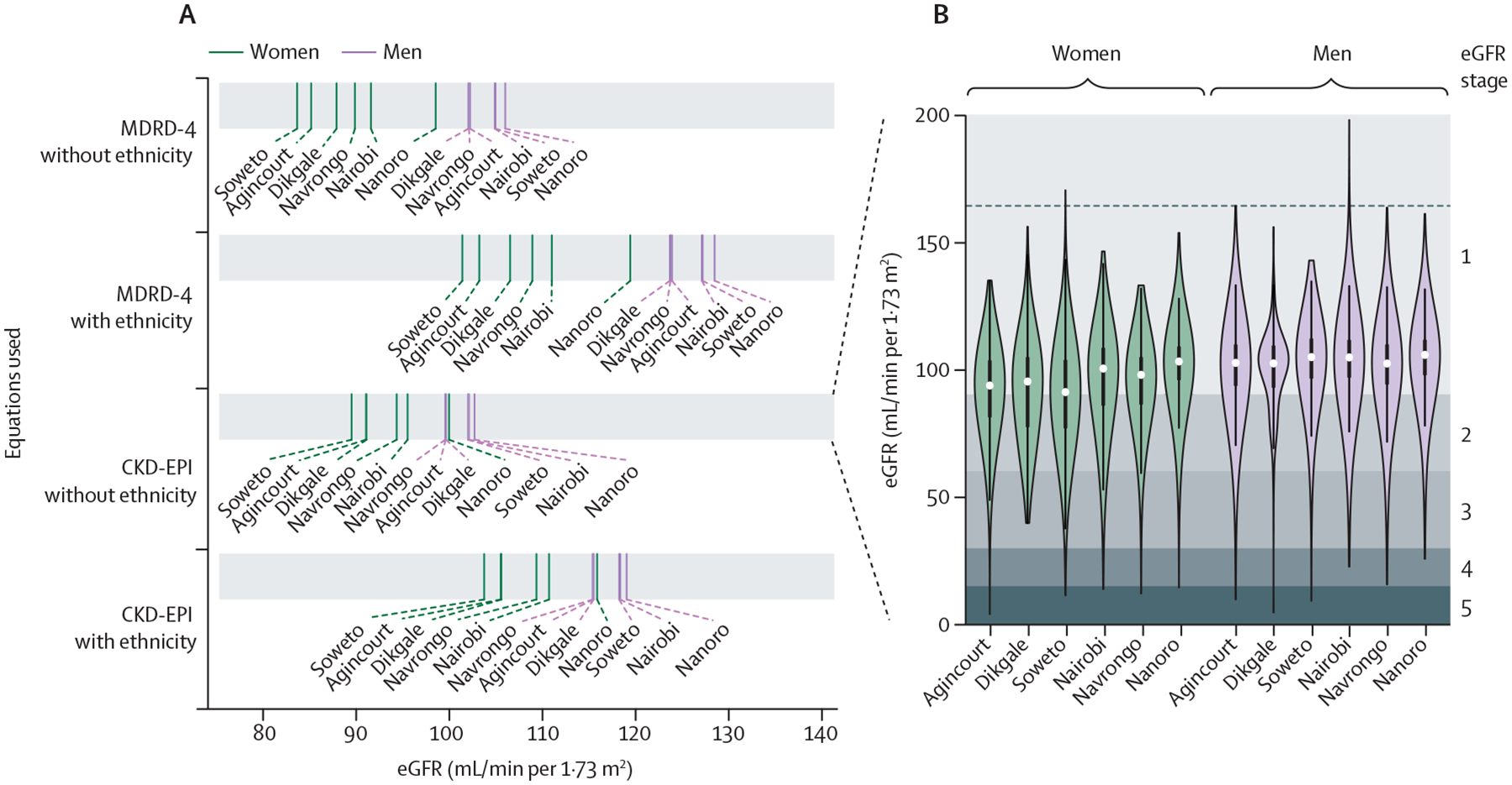
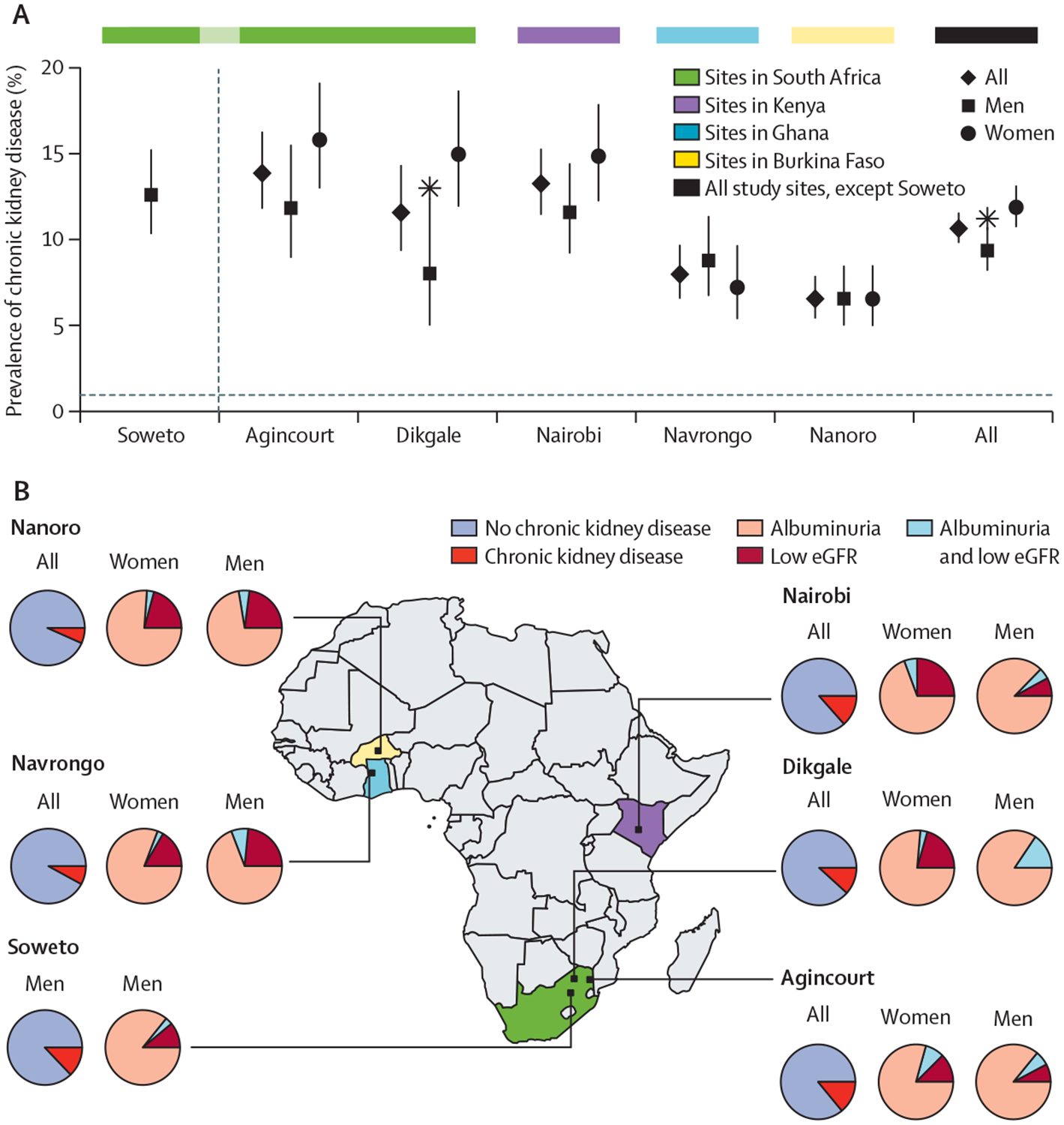
Methods: In this cross-sectional population study (Africa Wits-International Network for the Demographic Evaluation of Populations and their Health Partnership for Genomic Studies [AWI-Gen]), we recruited unrelated adult participants aged 40-60 years from four rural community research sites (Nanoro, Burkina Faso; Navrongo, Ghana; Agincourt and Dikgale, South Africa), and two urban community research sites (Nairobi, Kenya; and Soweto, South Africa). Participants were identified and selected using random sampling frames already in use at each site. Participants completed a lifestyle and medical history questionnaire, had anthropometric and blood pressure measurements taken, and blood and urine samples were collected. Markers of kidney damage were defined as low estimated glomerular filtration rate (eGFR; <60 mL/min per 1·73 m2), presence of albuminuria (urine albumin creatinine ratio >3 mg/mmol); or chronic kidney disease (low eGFR or albuminuria, or both). We calculated age-adjusted prevalence of chronic kidney disease, low eGFR, and albuminuria by site and sex and used logistic regression models to assess risk factors of kidney damage.
Findings: Between August, 2013, and August, 2016, we recruited 10 702 participants, of whom 8110 were analysable. 4120 (50·8%) of analysable participants were male, with a mean age of 49·9 years (SD 5·8). Age-standardised population prevalence was 2·4% (95% CI 2·1-2·8) for low eGFR, 9·2% (8·4-10·0) for albuminuria, and 10·7% (9·9-11·7) for chronic kidney disease, with higher prevalences in South African sites than in west African sites (14·0% [11·9-16·4] in Agincourt vs 6·6% [5·5-7·9] in Nanoro). Women had a higher prevalence of chronic kidney disease (12·0% [10·8-13·2] vs 9·5% [8·3-10·8]) and low eGFR (3·0% [2·6-3·6] vs 1·7% [1·3-2·3]) than did men, with no sex-specific differences for albuminuria (9·9% [8·8-11·0] vs 8·4% [7·3-9·7]). Risk factors for kidney damage were older age (relative risk 1·04, 95% CI 1·03-1·05; p<0·0001), hypertension (1·97, 1·68-2·30; p<0·0001), diabetes (2·22, 1·76-2·78; p<0·0001), and HIV (1·65, 1·36-1·99; p<0·0001); whereas male sex was protective (0·85, 0·73-0·98; p=0·02).
Interpretation: Regional differences in prevalence and risks of chronic kidney disease in sub-Saharan Africa relate in part to varying stages of sociodemographic and epidemiological health transitions across the area. Public health policy should focus on integrated strategies for screening, prevention, and risk factor management in the broader non-communicable disease and infectious diseases framework.
Funding: National Human Genome Research Institute, Office of the Director, Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institute of Environmental Health Sciences, the Office of AIDS Research, and National Institute of Diabetes and Digestive and Kidney Diseases, all of the National Institutes of Health, and the South African Department of Science and Technology.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests
SN, JAG, and JF report grants from Medical Research Council, South Africa; Newton; and GlaxoSmithKline outside of the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Chronic kidney disease in sub-Saharan Africa.Lancet Glob Health. 2019 Dec;7(12):e1587-e1588. doi: 10.1016/S2214-109X(19)30467-X. Lancet Glob Health. 2019. PMID: 31708128 No abstract available.
References
-
- Adeyi O, Smith O, Robies S. Public policy and the challenge of chronic noncommunicable diseases. Washington, DC: World Bank, 2007.
-
- Jha V, Garcia-Garcia G, Iseki K, et al. Chronic kidney disease: global dimension and perspectives. Lancet 2013; 382: 260–72. - PubMed
-
- Stanifer JW, Jing B, Tolan S, et al. The epidemiology of chronic kidney disease in sub-Saharan Africa: a systematic review and meta-analysis. Lancet Glob Health 2014; 2: e174–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
